Death is the one thing we all have in common, yet it's the one thing we’re terrible at talking about. Honestly, for most of us, "the end" is something we hope happens quietly in our sleep when we’re ninety-five. But for folks facing a terminal diagnosis, the conversation is way more urgent. You’ve probably heard a dozen different names for it—physician-assisted suicide, medical aid in dying (MAiD), death with dignity.
Whatever you call it, the legal map of the United States is changing fast.
📖 Related: Where is the Betty Ford Clinic? The Real Location of the World’s Most Famous Rehab
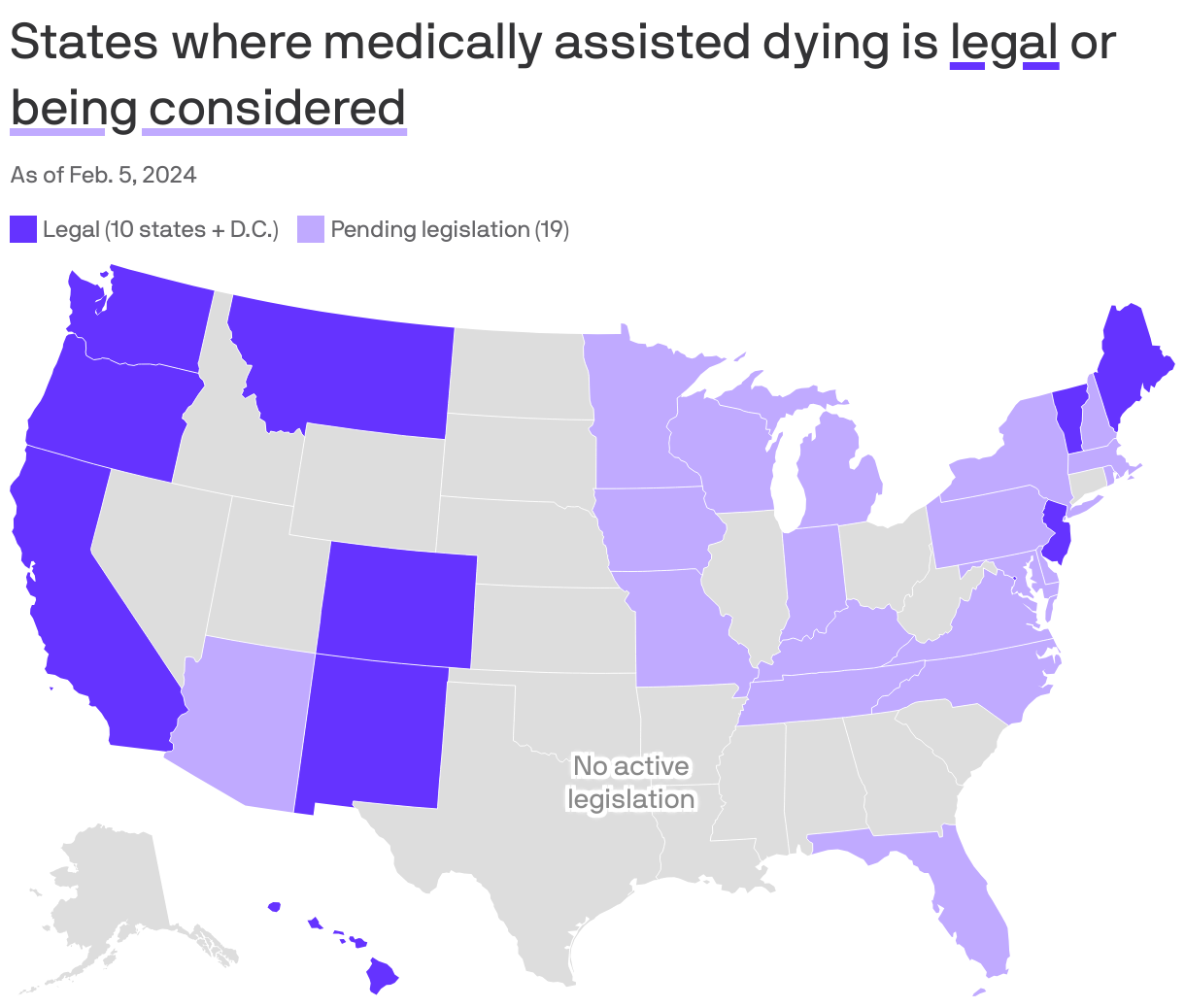
As of early 2026, the list of places where you can legally access medication to end your life has grown. It’s not just "that one law in Oregon" anymore. We’re looking at 12 states plus Washington, D.C., with New York currently on the verge of joining the group. But here’s the thing: just because a state is "legal" doesn't mean it's easy, and some of the biggest misconceptions involve who can actually cross state lines to get help.
The Current State of the Union on Assisted Death
If you’re looking for a quick roll call, here are the jurisdictions where which states allow assisted death currently applies:
- Oregon (The trailblazer, since 1994)
- Washington
- Montana (Legal via a 2009 court ruling, Baxter v. Montana, rather than a specific statute)
- Vermont
- California
- Colorado
- Washington, D.C.
- Hawaii
- New Jersey
- Maine
- New Mexico
- Delaware (The new kid on the block, fully effective in 2026)
- Illinois (Authorized in 2025)
New York is the "one to watch" right now. Governor Kathy Hochul signaled a massive shift in late 2025 by agreeing to sign the Medical Aid in Dying Act after years of legislative gridlock. It’s expected to be fully operational by mid-2026.
Why the "Where" Matters More Than You Think
It’s not enough to just live in a state that allows it. You've basically got to jump through a series of clinical hoops that would make a gymnast tired. Most states require you to be a resident. This is a huge point of contention. If you live in Florida or Texas and you're suffering, you can't just hop on a plane to New Jersey and get a prescription.
Wait—I should clarify.
There are two major exceptions to the residency rule now: Oregon and Vermont. Thanks to some intense lawsuits (like Gideonse v. Brown), these two states dropped their residency requirements. This means if you’re from a "non-legal" state, you could technically travel there. But—and this is a big "but"—you have to find a doctor in that state, do all your consultations there, and often physically stay there to ingest the medication. It’s a logistical nightmare for someone who is already very sick.
The "Six-Month" Rule and Other Strict Guardrails
Every single state law in the U.S. is built on the same foundation: you have to be terminal. This isn't like some of the laws in Belgium or the Netherlands where people with chronic mental illness or non-terminal disabilities might qualify.
🔗 Read more: Essential Oil for Fever: What the Science (and Your Grandma) Actually Says
In America, the rules are basically:
- 18+ years old.
- Mentally competent. This is huge. If you have advanced dementia or Alzheimer’s, you usually don't qualify because you can't "self-administer" or prove you're making a sound decision at the moment of the request.
- Six months or less to live. Two different doctors have to sign off on this prognosis.
- The "Self-Administer" Clause. This is the part that trips people up. The doctor doesn't give you a shot. They don't "do" it to you. They write a prescription for a powder (usually a mix of a cardiotonic, an opioid, and a sedative) that you have to mix with juice or applesauce and swallow yourself. If you can’t swallow or move your hands, you might not be eligible.
What Most People Get Wrong About the Process
People think it's like picking up a Z-Pak at CVS. It’s not.
In California, for instance, the End of Life Option Act was recently updated to shorten the waiting period, but it's still a process. You usually have to make two oral requests, sometimes 48 hours or 15 days apart (depending on the state), and one written request with witnesses.
And then there's the "opt-out" factor. Honestly, just because a state allows it doesn't mean your hospital does. Many Catholic-affiliated hospital systems—which make up a massive chunk of the U.S. healthcare landscape—strictly forbid their doctors from participating. You might live in a legal state, have a willing doctor, and then find out your hospice provider won’t let the medication on the premises.
The Cost Factor
Insurance is another headache. Since assisted death is still illegal at the federal level, Medicare won’t cover the drugs. Private insurance varies. Some people end up paying $500 to $1,000 out of pocket just for the medication itself, not to mention the doctor visits.
💡 You might also like: Can You Take Turmeric Everyday? The Truth About That Yellow Spice in Your Cabinet
The Ethical Tug-of-War
We can't talk about which states allow assisted death without mentioning why some people hate the idea. Groups like Not Dead Yet argue that these laws put disabled people at risk of being coerced into ending their lives because they feel like a "burden." On the flip side, organizations like Compassion & Choices argue that it’s the ultimate form of bodily autonomy.
The data from Oregon—which has been tracking this for 30 years—shows that most people who get the prescription actually have cancer (about 60-70%). Interestingly, about a third of the people who go through the whole process to get the meds never actually take them. Just having the bottle on the nightstand gives them enough peace of mind to keep going until they die naturally. It's a safety net, not a trap.
What’s Next if You’re Looking for Answers?
If you or a loved one are in a position where you’re looking into this, the first thing you need to do is check your local statutes. Laws change, and 2026 is seeing a lot of "improvement" bills—basically states trying to make the waiting periods shorter or allowing nurse practitioners to sign off instead of just MDs.
Actionable Steps to Take:
- Verify Residency: If you aren't in Oregon or Vermont, you almost certainly need to be a legal resident of the state where you're seeking help.
- Talk to Your Hospice: Don't wait until the last minute. Ask your hospice team directly: "Do you support medical aid in dying?"
- Find a Lead Doctor: Not every doctor is comfortable with this. You may need to find a "prescribing physician" and a "consulting physician" who are specifically willing to participate.
- Documentation: Start gathering your records now. You’ll need definitive proof of your diagnosis and prognosis from the last few months.
This isn't an easy path. It’s heavy, it’s bureaucratic, and it’s deeply personal. But knowing the actual map of which states allow assisted death is the first step in regaining some sense of control when everything else feels like it's spinning out.
Keep an eye on New York and Minnesota this year; the map is likely to look different by the time the summer rolls around.
Actionable Insight: If you live in a state where MAiD is not yet legal, your best resource for navigating out-of-state travel is the American Clinicians Academy on Medical Aid in Dying. They provide updated clinical guidelines on which providers in Oregon and Vermont are currently accepting out-of-state terminal patients.