Death is uncomfortable. People don't like talking about it over dinner, but when you're facing a terminal diagnosis, it becomes the only conversation that matters. Right now, there’s a massive patchwork of laws across the U.S. that determines whether you have the "right to die" or if you're legally required to wait for nature to take its course. It’s a mess.
If you're searching for states allow assisted death, you're likely looking for "Medical Aid in Dying" (MAID). That’s the clinical term. It isn't "suicide" in the traditional sense—at least not according to the laws in place. It’s a medical protocol. You have to be terminally ill. You have to be mentally competent. And, crucially, you have to be in the right zip code.
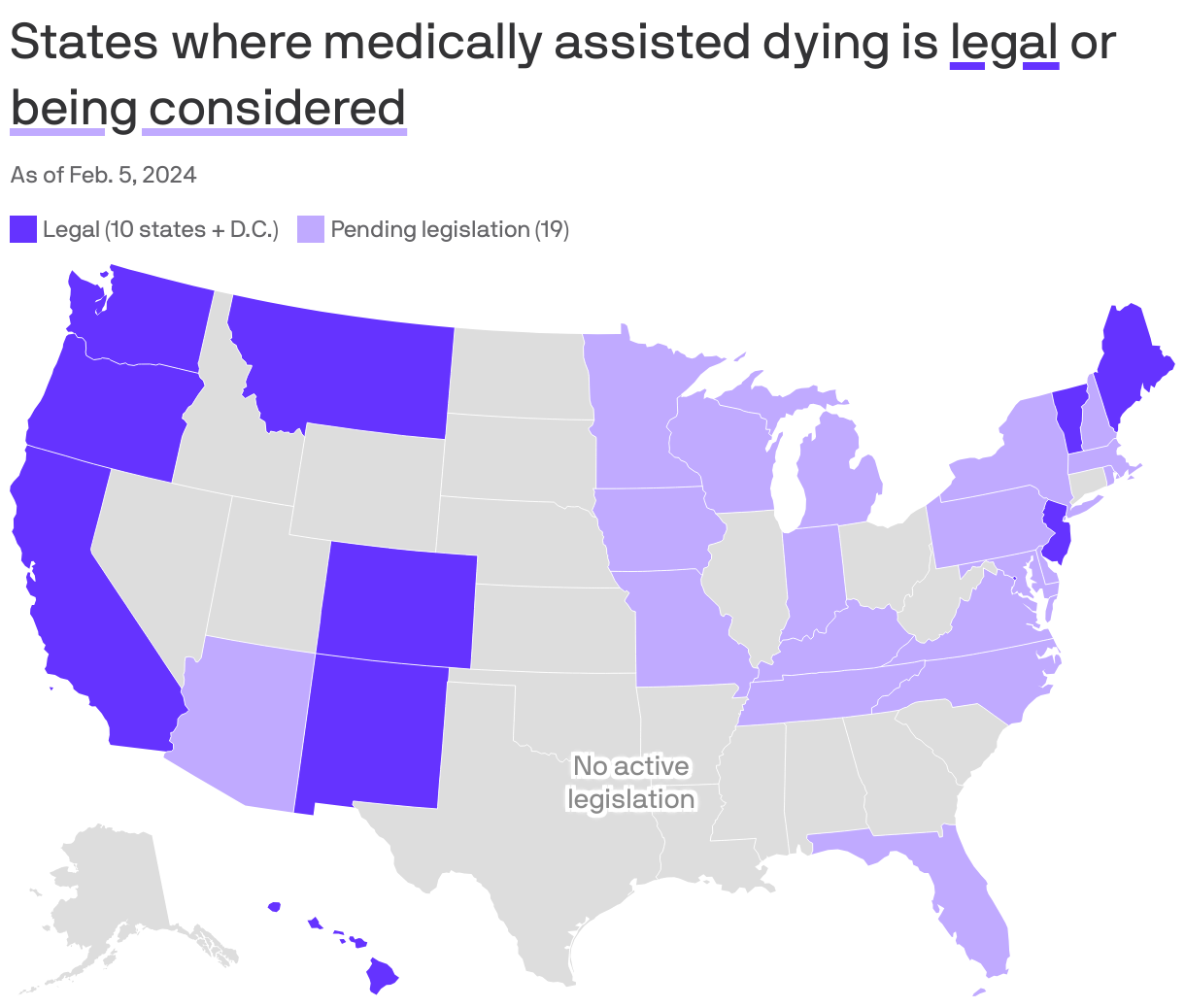
The Current Map: Where it’s Legal Right Now
Ten states and the District of Columbia have legalized this. It started with Oregon back in 1997. People thought the sky would fall. It didn't. Since then, a slow trickle of other states followed suit.
Washington joined in 2008. Then Vermont. California passed its law in 2015, which was a huge turning point because of the sheer population size. Colorado, Hawaii, Maine, New Jersey, and New Mexico are also on the list. Most recently, we've seen movements in places like Minnesota, though the legislative battles there are often brutal and move at a snail's pace.
Montana is the weird outlier. They don't have a specific statute passed by the legislature. Instead, a 2009 State Supreme Court ruling (Baxter v. Montana) basically said that nothing in state law prohibits a doctor from honoring a terminally ill patient's request for life-ending medication. It’s legal, but it’s "legal-ish" in a way that makes some doctors nervous because there aren't the same rigid regulatory frameworks you find in Oregon or California.
The "Residency" Problem is Vanishing
For a long time, you had to be a resident of the state to use these laws. You couldn't just fly to Portland, check into a hotel, and ask for a prescription. That’s changing.
🔗 Read more: In the Veins of the Drowning: The Dark Reality of Saltwater vs Freshwater
Oregon and Vermont have recently settled lawsuits that challenged the residency requirement. Basically, they've stopped enforcing it. This is a massive shift. It means a patient from Idaho—where assisted death is strictly illegal—could theoretically travel to Oregon to access the medication. However, it’s not as simple as a weekend trip. You still need two doctors to sign off, and many clinicians are hesitant to work with out-of-state patients because of the legal "gray zone" regarding bringing the medication back across state lines. Don't do that. Crossing state lines with federally controlled substances intended for this purpose is a legal nightmare.
How the Process Actually Works
It isn't a "push a button and it’s over" scenario. The process is intentionally cumbersome. They want to make sure you aren't being coerced by a greedy heir or acting on a temporary bout of depression.
First, you need a terminal diagnosis. Usually, that means a doctor has certified you have six months or less to live. Think Stage IV cancer, ALS, or advanced heart failure.
You have to make two oral requests, usually 15 days apart. Then a written request with witnesses. Then a second doctor has to confirm the diagnosis and your mental capacity. If a doctor thinks you’re depressed in a way that’s clouding your judgment—rather than just being understandably sad that you’re dying—they’ll refer you to a psychiatrist.
The Self-Administration Rule
This is the part most people get wrong. In every single one of the states allow assisted death, the patient must be able to self-administer the drug. The doctor doesn't give you an injection. They don't put it in your IV. They write a prescription for a powder (usually a mix of barbiturates or a specific "cocktail" of meds like D-DMA: Digoxin, Diazepam, Morphine, and Amitriptyline).
💡 You might also like: Whooping Cough Symptoms: Why It’s Way More Than Just a Bad Cold
You have to be able to swallow it or, if you have a feeding tube, push the plunger yourself. If you lose the physical ability to swallow before the waiting period is up, you're out of luck. This is a heartbreaking reality for many ALS patients who wait too long.
The Massive Divide: Ethics and Opposition
Not everyone thinks this is progress. Not by a long shot.
The Catholic Church and several disability rights groups, like "Not Dead Yet," argue that these laws create a "duty to die." They worry that elderly or disabled people will feel like a burden on their families and choose death not because they want it, but because they feel they should.
There’s also the "slippery slope" argument. Critics point to Canada’s MAID system, which is much broader than the U.S. system. In Canada, you don't necessarily need to be "terminal" in the six-month sense; you just need "unbearable suffering." U.S. laws are much tighter, but the fear remains that once you open the door, it stays open.
On the flip side, proponents like the organization Compassion & Choices argue that this is the ultimate form of bodily autonomy. They point to data from Oregon’s annual reports showing that a huge percentage of people who get the prescription never actually use it. Just having the bottle on the nightstand provides enough peace of mind to keep going. It’s an insurance policy against a "bad death."
📖 Related: Why Do Women Fake Orgasms? The Uncomfortable Truth Most People Ignore
Real-World Nuance: The Cost and the Access
Let's talk money and logistics, because nobody mentions this. Even in states allow assisted death, finding a doctor who will actually do it is hard.
Many Catholic-affiliated hospital systems (like Providence or Dignity Health) forbid their doctors from participating. A doctor in a rural part of Washington might be "allowed" by law to help you, but if their employer says no, they can’t. You might have to drive four hours to a different health system.
Then there’s the cost. The medications aren't cheap. We're talking anywhere from $500 to $3,000. Since the drugs are used for a purpose not recognized by federal law, Medicare won't cover them. Some private insurances do, but many don't. You're often paying out of pocket for the right to end your life on your own terms.
What to Do If You’re Navigating This
If you or a loved one are in one of the states allow assisted death, or considering traveling to one, you need to start the conversation early. Like, months earlier than you think.
- Find a supportive physician immediately. Ask your oncologist or primary care doctor directly: "Do you participate in the Death with Dignity Act?" If they say no, ask if they will at least refer you to someone who does.
- Check your hospice. Some hospices are very supportive and will have nurses present (though they can't "help" with the meds). Others will drop you as a patient if you choose this route.
- Get your paperwork in order. Ensure your Advanced Directive is crystal clear.
- Consult a specialist. Organizations like the American Clinicians Academy on Medical Aid in Dying provide actual clinical guidelines and can sometimes help find participating doctors.
The legal landscape is shifting. Bills are currently being debated in New York, Massachusetts, and several other states. But as of today, your geography is your destiny when it comes to end-of-life choices.
Essential Next Steps for Families
- Review the specific statute for your state. Oregon’s rules are slightly different from New Jersey’s regarding waiting periods (NJ requires a 15-day wait between oral requests).
- Talk to a pharmacist. Not every pharmacy stocks these medications. You usually need a specialized compounding pharmacy.
- Document everything. Ensure the "voluntary" nature of the request is documented in the medical record to protect your family and your doctors from any potential legal blowback later.
Accessing these laws requires a level of administrative energy that many terminal patients simply don't have. If this is the path you want, you need an advocate—a family member or friend—who is willing to handle the phone calls, the paperwork, and the logistical hurdles while you focus on the time you have left.