So, you’ve got the envelope. Or maybe just a login to a patient portal where a grainy, black-and-white bulging disc mri image is staring back at you. It looks scary. Honestly, the first time most people see their own spine on a screen, they assume they’re one wrong move away from permanent damage. The dark spots, the little protrusions pushing against the white space—it feels like a smoking gun for your back pain.
But here is the weird thing about spinal imaging: what you see isn't always why you hurt.
I’ve spent years looking at these scans and talking to neurosurgeons like Dr. Kevin Pauza or researchers who study the "mismatch" between imaging and reality. There is a massive gap between a "finding" on a piece of film and a "diagnosis" of why your leg is tingling or your lower back feels like it’s in a vice. We need to talk about what that bulging disc mri image actually represents, because for a lot of you, that bulge has been there for a decade and isn't the reason you're hurting today.
What You’re Actually Seeing on the Screen
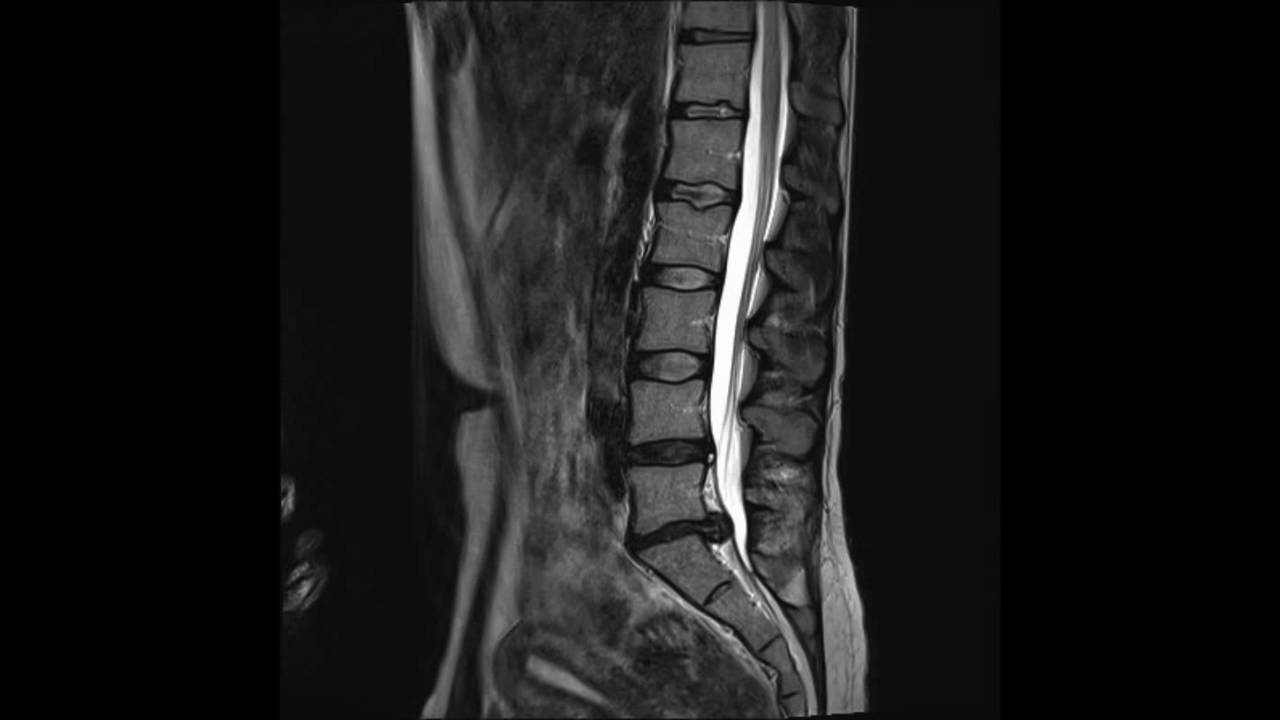
When you look at a T2-weighted MRI—that’s the one where the spinal fluid looks bright white—your discs should look like plump, white marshmallows with a dark ring around them. The white part is water. It’s hydration. It’s shock absorption.
A bulging disc happens when that "marshmallow" starts to lose water and sags. Imagine taking a jelly donut and pressing down on the top with your palm. The sides of the dough push out evenly in all directions. That is a bulge. It is symmetrical. It is usually a sign of "wear and tear" or what doctors call degenerative disc disease, which, let’s be real, is a terrible name because it’s often just a normal part of getting older.
It’s different from a herniation. In a herniation, the "jelly" actually squirts out through a crack. On a bulging disc mri image, the outer layer (the annulus fibrosus) is still intact. It’s just... overextended.
The Sagittal vs. Axial View
You’ll usually see two main angles. The sagittal view is the side profile. It looks like a map of your profile from the side. This is where you see the "stack" of vertebrae. If you see a disc poking backward into the white canal where the nerves live, that’s your bulge.
The axial view is different. It’s like the MRI sliced you in half like a loaf of bread and is looking down from the top. This is the view that actually matters for your symptoms. Why? Because it shows the "exit doors"—the neuroforamen. If your bulging disc mri image shows the disc material encroaching on those tiny holes where the nerves exit the spine, that’s when you start feeling the lightning bolts in your calf.
👉 See also: Nuts Are Keto Friendly (Usually), But These 3 Mistakes Will Kick You Out Of Ketosis
The "Incidental Finding" Problem
Here is a statistic that usually shocks people: A study published in the American Journal of Neuroradiology looked at 3,110 people who had zero back pain. None. They were perfectly fine.
The researchers found that 30% of 20-year-olds had disc bulges. By the time they looked at 80-year-olds, 84% had them.
Think about that.
If you are 40 years old, there is basically a 50/50 chance that if we threw you in an MRI machine right now, we’d find a bulging disc, even if you feel like a million bucks. This is why doctors get annoyed with "MRI-based medicine." If a clinician just looks at your bulging disc mri image without testing your reflexes or asking where your pain goes, they might try to "fix" a bulge that was already there when you were 25 and doing gymnastics.
The image is a snapshot. It isn't a movie. It doesn't show inflammation, and inflammation is often the real villain. A disc can bulge and touch a nerve, but if there’s no chemical inflammation, you might not feel a thing. Conversely, a tiny bulge that is highly inflamed can make you want to scream.
Why Your Radiologist Uses Such Scary Language
"Multilevel degenerative changes."
"Loss of disc height."
"Effacement of the thecal sac."
Reading an MRI report feels like reading a horror novel. Radiologists are paid to be hyper-thorough. They have to list every single "abnormality" they see, even if it has no clinical significance. When they see a bulging disc mri image, they note it. They don't know if you're an Olympic powerlifter or someone who can't walk to the mailbox.
✨ Don't miss: That Time a Doctor With Measles Treating Kids Sparked a Massive Health Crisis
When you see "effacement of the thecal sac," it basically means the bulge is touching the "bag" that holds your spinal fluid and nerves. It sounds like your spine is collapsing. Usually, it just means things are a bit crowded in there. It’s like a crowded subway car; just because someone is leaning against you doesn’t mean they’re breaking your ribs.
When the Image Actually Matches the Pain
So, when should you actually worry about that bulging disc mri image?
Context is everything. If the image shows a bulge at the L5-S1 level (the very bottom of your spine) and it is specifically pushing on the right side, and you have pain running down your right buttock into your big toe... okay, now we have a match.
We look for "correlation."
- Neurological deficits: Is your foot dragging? Can you not stand on your tiptoes? If the image shows a bulge compressing a nerve and your muscles are actually failing, that’s a "red flag" scenario.
- Cauda Equina symptoms: This is rare, but if your MRI shows a massive bulge and you’re losing control of your bladder or have "saddle anesthesia" (numbness where a bike seat would touch you), stop reading this and go to the ER. The image matters a lot there.
- Progressive worsening: If the pain is getting worse despite physical therapy, the MRI helps surgeons decide exactly where to put the needle or the scalpel.
Can a Bulging Disc Heal?
People think a bulge is permanent. Like a dent in a car door.
Actually, the body is kind of amazing at cleaning this stuff up. While herniations (the "jelly out" kind) actually heal faster because the immune system can "see" the leaked material and eat it away, bulges can also regress. When you improve your core stability and change your posture, you change the pressure on that disc.
Sometimes the bulging disc mri image doesn't change, but the pain goes away. Why? Because the inflammation died down. The nerve got used to its new neighbor. The "chemical soup" of cytokines and prostaglandins that makes nerves hypersensitive evaporated.
🔗 Read more: Dr. Sharon Vila Wright: What You Should Know About the Houston OB-GYN
Don't get obsessed with getting a "clean" follow-up MRI. It’s a waste of money. Focus on how you move.
Better Ways to Handle the Results
If you're staring at your scan right now, take a breath. You aren't "broken." You have a spine that has lived a life.
First, get a second opinion from someone who isn't a surgeon. Surgeons are trained to find things to cut. That’s their job. Talk to a physical therapist or a physical medicine doctor (physiatrist). Ask them: "Does this bulging disc mri image explain my specific symptoms, or is this just what a 40-year-old spine looks like?"
Second, look at your lifestyle. Disc bulges hate two things: sitting for 10 hours a day and dehydration. Discs are like sponges. They need movement to pump nutrients in and out. If you sit still, the disc doesn't get "fed," it sags, and the bulge looks worse on the screen.
Third, stop Googling "spine surgery." Most disc issues—bulges included—resolve with "conservative management" within 6 to 12 weeks. That means walking, specific exercises (like the McGill Big Three), and maybe some anti-inflammatories.
Actionable Steps for Your Next Appointment
Don't just walk into your doctor's office and say, "My back hurts." You need to be the expert on your own body to help them interpret that bulging disc mri image correctly.
- Map your pain: Exactly where does it go? Does it stop at the knee? Does it go to the pinky toe? Different nerves correspond to different discs. If your pain doesn't match the disc on the MRI, the disc isn't the problem.
- Test your strength: Can you do a calf raise on one leg? Can you pull your big toe toward your face against resistance? Record this.
- Ask for the "Clinical Correlation": Use that specific phrase with your doctor. Ask, "How does this bulge correlate with my physical exam?" If they can't give you a straight answer, they are just treating a picture, not a person.
- Request a copy of the actual images: Not just the report. Sometimes seeing the "axial view" yourself helps you realize that the "nerve compression" mentioned is actually just a tiny bit of contact.
Ultimately, your MRI is just one piece of a puzzle. It’s a blueprint, but the blueprint isn't the house. You can have a messy blueprint and still have a very sturdy, functional home. Treat your movement, treat your strength, and don't let a gray smudge on a screen dictate your quality of life.