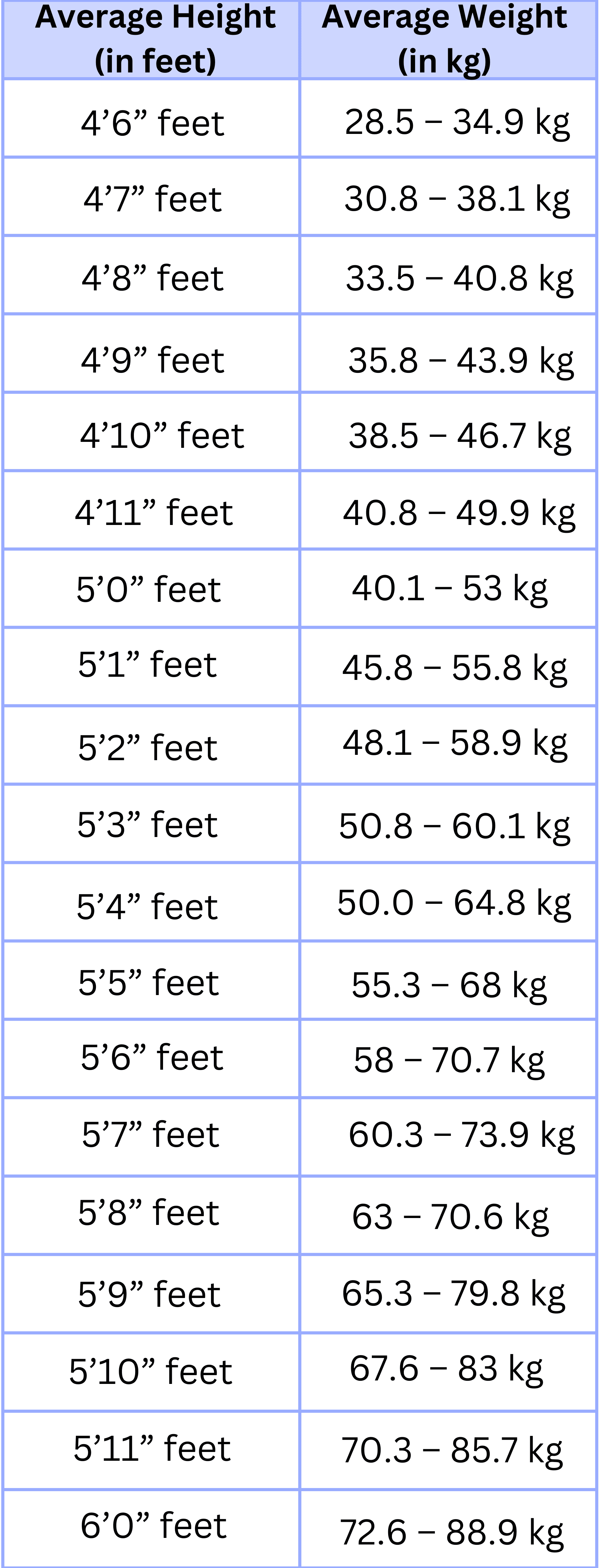
You’ve seen the chart. It’s usually hanging on a fading piece of paper in a sterile exam room, or maybe you stumbled across a digital version while spiraling down a late-night health rabbit hole. It tells you that if you are five-foot-nine and forty years old, you should weigh exactly X. If you weigh Y, the chart turns red. You feel like you've failed a test you didn't even know you were taking.
But here is the thing.
The concept of normal weight for height and age is actually way more "gray area" than most medical websites want to admit. We have been conditioned to worship the Body Mass Index (BMI) as the gold standard of health, yet the guy who invented it, Adolphe Quetelet, specifically said it wasn't meant to measure individual health. He was a mathematician, not a doctor. He was looking at populations, not the person standing on the scale in their underwear feeling bad about a slice of pizza.
The BMI trap and why it misses the mark
Most people looking for their normal weight for height and age start with the BMI formula. It’s simple math. You take your weight, divide it by your height squared, and boom—you’re labeled. Underweight. Normal. Overweight. Obese.
It's efficient. It’s fast. It’s also kinda lazy.
BMI doesn't know if you’re a marathon runner with legs like tree trunks or someone who hasn't lifted a weight since the Bush administration. Muscle is dense. It’s heavy. If you have a high muscle-to-fat ratio, the BMI scale will flag you as overweight or even obese. This isn't just a theoretical problem for bodybuilders. Research published in the International Journal of Obesity has shown that nearly half of people classified as "overweight" by BMI are actually metabolically healthy when you look at their blood pressure, cholesterol, and insulin resistance.
So, what are we actually looking for?
Usually, when we talk about "normal," we mean a weight that doesn't put us at a higher risk for chronic stuff like Type 2 diabetes or heart disease. But age changes the math in ways those 1950s-era charts rarely account for.
Age is the variable nobody talks about enough
As you get older, your body's relationship with weight shifts. It's not just about the metabolism slowing down—though that's real and annoying—it's about where the weight goes and what it's made of.
✨ Don't miss: The Truth Behind RFK Autism Destroys Families Claims and the Science of Neurodiversity
When you're twenty, you can carry a few extra pounds and your joints barely notice. When you’re sixty, that same weight might be the difference between hiking with your grandkids and needing a knee replacement. However, there is a weird phenomenon called the "obesity paradox" in geriatrics. Studies, including those cited by the Journal of the American Medical Association, suggest that for folks over 65, carrying a little extra weight (being in the "overweight" category of 25 to 29.9 BMI) might actually be protective. It provides a reserve of energy if you get sick and helps prevent osteoporosis.
Basically, being "too thin" becomes a bigger risk factor for mortality in the elderly than being slightly "heavy."
The shift in body composition
Let's talk about sarcopenia. It sounds like a Greek tragedy, and for your muscles, it kinda is. Starting around age 30, you begin losing muscle mass if you aren't actively fighting to keep it. You might stay the exact same weight on the scale from age 30 to age 50, but your body composition has completely flipped. You have less muscle and more visceral fat—that's the deep belly fat that wraps around your organs.
This is why normal weight for height and age is a moving target.
A 50-year-old woman weighing 150 pounds might have a much higher body fat percentage than she did at 150 pounds when she was 22. The scale stays the same. The health risk goes up. This is often called "skinny fat" or metabolically obese normal weight (MONW). It’s sneaky. It’s why looking at the number on the scale without looking at your waist circumference or your strength levels is basically useless.
Height: The vertical reality
Height is the most fixed part of the equation, but even that gets wonky. Most charts assume a linear relationship between height and weight, but bodies are three-dimensional objects.
Tall people often get screwed by standard weight charts. Because BMI squares height ($h^2$), it tends to overstate "fatness" in tall people and understate it in short people. A guy who is 6'4" might be told he is overweight even if he’s quite lean, simply because the math doesn't scale perfectly for human proportions.
Then there is the frame size issue.
🔗 Read more: Medicine Ball Set With Rack: What Your Home Gym Is Actually Missing
You’ve probably heard someone say they are "big-boned." People usually roll their eyes at that, but it’s a real biological thing. Your bone structure—the width of your elbows, wrists, and shoulders—determines how much weight your frame can naturally support. A person with a "large" frame can easily weigh 15-20 pounds more than someone of the same height with a "small" frame and have the exact same body fat percentage.
Better ways to measure than just the scale
If we are going to move past the obsession with normal weight for height and age as a single number, we need better tools. None of these are perfect, but they offer a clearer picture of what’s actually happening under the skin.
- Waist-to-Hip Ratio (WHR): This is often a better predictor of heart disease than BMI. If you carry your weight in your belly (the "apple" shape), you're at higher risk than if you carry it in your hips and thighs (the "pear" shape).
- Waist-to-Height Ratio: A simple rule of thumb is that your waist circumference should be less than half your height. It's shockingly accurate for assessing health risk across different ages and ethnicities.
- DEXA Scans: Once only used for bone density, these are now the gold standard for measuring body fat versus lean mass. They are expensive, but they don't lie.
- The "Pants Test": Honestly? How your clothes fit and how much energy you have often tell you more than a scale ever will.
The role of genetics and ethnicity
We also have to acknowledge that the "normal" ranges were largely built on data from Caucasian populations of European descent. This is a massive flaw.
Research has shown that people of South Asian descent, for instance, have a higher risk of developing diabetes at a much lower BMI than Caucasians. For this population, a BMI of 23 might be the "tipping point" for health issues, whereas for a white person, that point might be 25 or 27. Conversely, some studies suggest that people of African descent may have higher bone density and muscle mass, meaning a higher BMI doesn't necessarily translate to the same health risks.
The medical community is slowly—very slowly—starting to adopt "ethnic-specific" BMI cutoffs. But until that becomes mainstream, you have to be your own advocate. You have to ask your doctor to look at your blood work, not just your height and weight chart.
What actually matters for your longevity
If you’re obsessing over hitting a specific "normal" number, you’re probably missing the forest for the trees.
Health isn't a destination; it's a set of metabolic markers. You can be at a "normal" weight and have sky-high blood sugar because you live on soda and stress. You can be "overweight" and have the cardiovascular fitness of an athlete.
Real health looks like this:
💡 You might also like: Trump Says Don't Take Tylenol: Why This Medical Advice Is Stirring Controversy
- Blood pressure regularly under 120/80.
- Resting heart rate in a range that shows your heart isn't working overtime.
- Fastened blood glucose levels that aren't creeping into the pre-diabetic range.
- The ability to carry your own groceries or climb three flights of stairs without feeling like you're dying.
Actionable steps for finding your "personal" normal
Instead of chasing a phantom number on a 1990s PDF, try these specific shifts in how you track your body.
Focus on "Power-to-Weight" ratio. Instead of trying to lose 10 pounds, try to get stronger. If you can lift more, walk faster, or hold a plank longer while staying the same weight, you have effectively changed your body composition. You have replaced "unhealthy" weight with "functional" weight. This is the ultimate goal as you age.
Measure your waist, not just your mass. Get a soft measuring tape. Measure at the narrowest part of your torso (usually right above the belly button). If you are a woman and that number is over 35 inches, or a man and it’s over 40, that is a much bigger red flag than whatever the scale says. Visceral fat is the real enemy.
Track your trends, not your daily fluctuations. Your weight can swing 3 to 5 pounds in a single day based on salt intake, hydration, and even how much you slept. If you must weigh yourself, do it once a week at the same time and look at the moving average over a month.
Prioritize protein and resistance training. Since age-related muscle loss is the biggest threat to a "normal" healthy weight, you have to fight back. Eat more protein than you think you need—aim for roughly 0.7 to 1 gram per pound of goal body weight—and lift something heavy at least twice a week.
Get a full metabolic panel. The next time you see your doctor, don't just talk about weight. Ask for an A1C test (to see average blood sugar over three months) and a full lipid panel. If these numbers are great, the number on the scale is a lot less urgent.
Weight is a data point. It is not the whole story. Your "normal" weight is the one that allows you to live a life full of movement and free of chronic medication, regardless of what the chart on the wall says. Stop trying to fit into a box that wasn't built for your specific biology. Focus on the metrics that actually correlate with a long, vibrant life.