Honestly, if you ask someone on the street about tuberculosis, they usually think of two things: Victorian poets coughing into silk handkerchiefs or a disease that vanished in the 1950s. Neither is true. TB is very much alive, and in 2026, it remains the world's deadliest infectious killer, recently reclaiming that grim title from COVID-19. But the real question—the one that actually matters if you're staring at a positive test result—is: is tb curable now?
The short answer is a resounding yes. It’s absolutely curable.
But "curable" doesn't mean "easy." We aren't talking about a three-day course of Z-Pak. Dealing with Mycobacterium tuberculosis is a marathon, not a sprint. The bacteria are stubborn, slow-growing, and frankly, kind of brilliant at hiding inside your own immune cells. However, thanks to some massive breakthroughs in the last two years, the "marathon" just got a lot shorter.
The 2026 Reality: Shortening the Long Road
For decades, the standard treatment for a "basic" case of TB was six months of four different drugs. You had to take them every single day. If you felt better after two months and stopped? The bacteria would come roaring back, often stronger than before.
But things changed. In early 2025, the World Health Organization (WHO) and the CDC officially shifted their stance. For many people with drug-susceptible TB, we’ve moved from a 6-month grind to a 4-month regimen.
This newer 4-month treatment typically uses a combination of rifapentine, moxifloxacin, isoniazid, and pyrazinamide. It's a heavy hitter. The goal here is simple: kill the bacteria faster so patients don't drop out of treatment. Because let’s be real, remembering to take pills for half a year is a huge ask, especially when you start feeling "fine" after the first few weeks.
Why You Can’t Just Quit Early
There is this dangerous moment in TB treatment. It usually happens around week four. You stop coughing. Your fever vanishes. You gain back the weight you lost. You feel like a human again.
This is exactly when the bacteria are most dangerous.
👉 See also: Happy Medical Assistant Day: Why These Heroes Are the Real Glue of Modern Healthcare
TB bacteria are "persisters." Some of them go into a sort of deep sleep where most antibiotics can't touch them. If you stop taking your meds because you feel okay, those sleeping bacteria wake up. And when they wake up, they’ve "learned" how to fight the drugs you were using. That’s how we get drug-resistant TB, which is a whole different beast.
Is TB Curable Now if it’s Drug-Resistant?
This used to be the nightmare scenario. If you had Multidrug-Resistant TB (MDR-TB) five or ten years ago, you were looking at 18 to 24 months of treatment. We're talking thousands of pills and daily, painful injections that could cause permanent hearing loss or kidney failure. It was brutal.
In 2026, that "horror story" version of treatment is becoming obsolete.
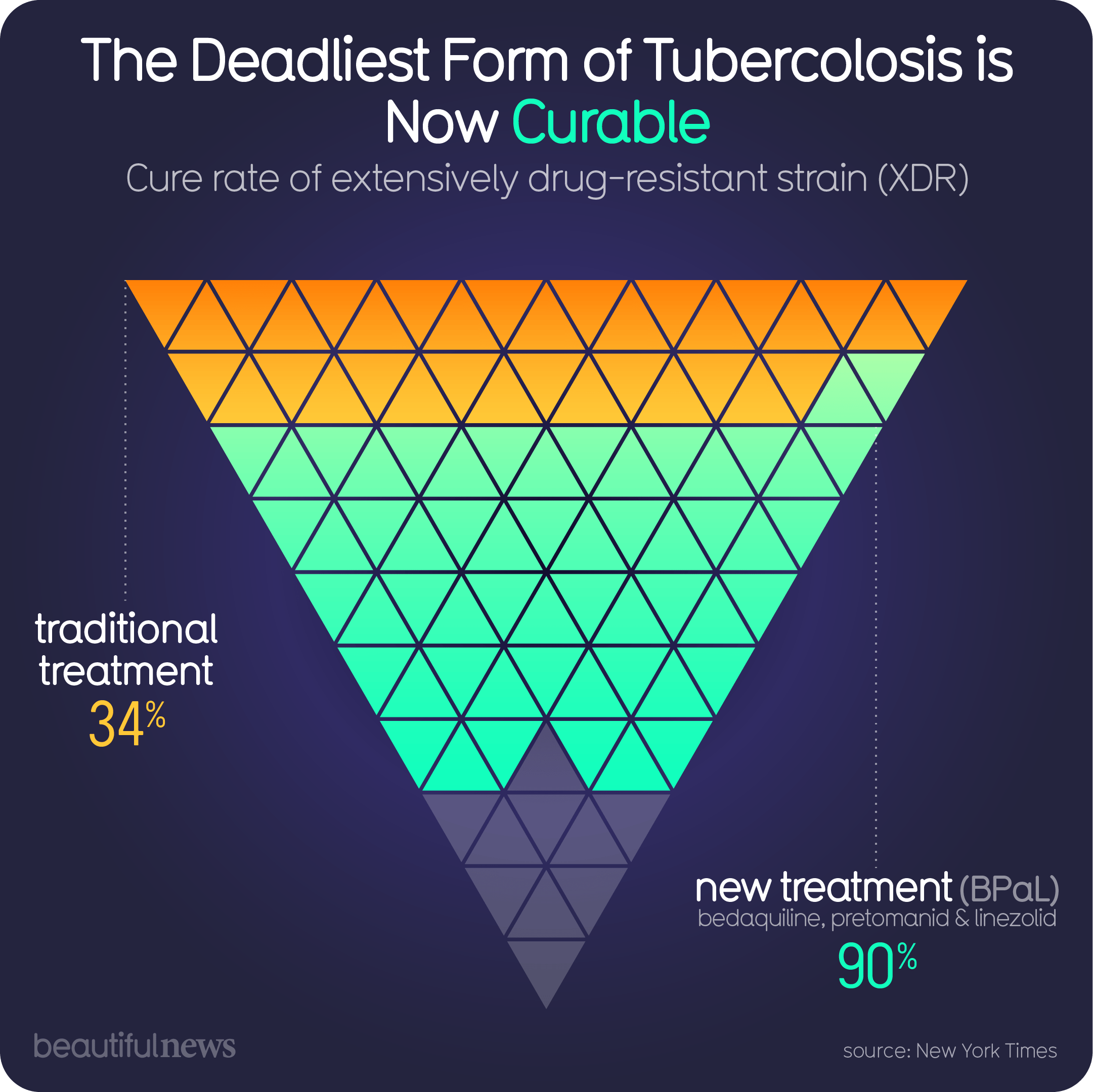
The hero of this story is a regimen called BPaLM. It sounds like a tech startup, but it stands for a cocktail of four drugs: Bedaquiline, Pretomanid, Linezolid, and Moxifloxacin.
- Duration: 6 months (down from 2 years).
- Method: All-oral. No more needles.
- Success Rate: Clinical trials and recent data from the TB-PRACTECAL study show success rates around 89-90%.
That is a game-changer. We are seeing people with "untreatable" strains walking out of clinics healthy in six months. It’s arguably the biggest win in pulmonary medicine this decade.
The Latent TB Loophole
Most people don't realize that about one-fourth of the world's population has "latent" TB. This means the bacteria are in your body, but they're dormant. You aren't sick, and you aren't contagious.
Is latent TB curable? Yes, and you should cure it.
If you have a weakened immune system—maybe from age, diabetes, or medications—that "sleeping" TB can wake up and become active disease. Modern "preventive" treatments like the 3HP regimen (isoniazid and rifapentine once a week for 12 weeks) make it incredibly easy to clear the infection before it ever makes you sick. Honestly, if you've ever lived in a high-burden area, getting screened for latent TB is just common sense.
What About a Vaccine?
You probably got the BCG vaccine as a kid if you grew up outside the US. It’s okay, but it mostly protects children from severe brain-related TB. It doesn't do much for adults with lung TB.
As of early 2026, we are in a bit of a "waiting room" for the next generation of vaccines. The M72/AS01E candidate is currently in Phase 3 trials. Early data suggests it's about 50% effective at preventing active disease in adults. While 50% doesn't sound like a miracle, in the world of TB, it would save millions of lives. We’re also seeing progress with MTBVAC, which is the first live-attenuated vaccine derived from a human strain.
We aren't there yet, but for the first time in a century, the pipeline is actually full.
The Practical "Next Steps" If You’re Worried
If you’re asking "is tb curable now" because you or someone you love is symptomatic, here is the expert-level reality check.
1. Get a Molecular Test, Not Just a Smear
Older tests (sputum smears) miss about half of all cases. Insist on a Rapid Molecular Test like GeneXpert. It doesn’t just tell you if you have TB; it tells you instantly if your version is resistant to common drugs like Rifampicin. This saves weeks of guesswork.
2. Side Effects are Manageable
The drugs can be tough. Isoniazid can cause tingling in the hands (peripheral neuropathy), but taking Vitamin B6 usually stops it. Bedaquiline requires monitoring your heart rhythm (EKG). Don’t suffer in silence—tell your doctor, because there are almost always ways to tweak the dose.
3. Nutrition is a Medication
TB eats your body's resources. In 2025, programs like India's Ni-kshay began providing "Energy Dense Nutritional Supplementation." Basically, if you aren't eating enough protein and calories, the drugs have a harder time working. Treat your meals as part of your prescription.
4. The Support Factor
Treatment failure isn't usually a failure of medicine; it's a failure of logistics. Look for DOTS (Directly Observed Treatment, Short-course) or digital tools that help you stay on track. There's no shame in needing a reminder for a 6-month pill course.
The bottom line for 2026? Tuberculosis is no longer the life sentence it once was. Between the 4-month regimens for standard cases and the 6-month BPaLM "miracle" for resistant cases, the tools to end this disease are finally in our hands. The cure exists. You just have to finish the bottle.
Actionable Takeaways for Patients and Caregivers
- Confirm the Strain: Ensure your doctor has performed drug-susceptibility testing (DST) so you aren't taking the wrong meds.
- Monitor Liver Health: TB drugs are processed by the liver. Avoid alcohol entirely during treatment and watch for yellowing of the eyes (jaundice).
- Contact Tracing: If you have active TB, everyone in your household needs a skin or blood test (IGRA) immediately.
- Advocate for the Shorter Course: Ask your provider if you are eligible for the 4-month rifapentine-moxifloxacin regimen rather than the older 6-month standard.