Finding the right glp-1 dosage for weight loss isn't as simple as just picking a number and hoping for the best. It’s a slow burn. Most people think they can just jump straight to the high dose and watch the pounds melt away, but that's a fast track to spending your entire weekend on the bathroom floor. Honestly, the way these medications are marketed makes it sound like magic, but the biology of how your body handles these peptides is actually pretty finicky.
You've probably heard of names like Ozempic, Wegovy, or Zepbound. They all fall under the GLP-1 (glucagon-like peptide-1) receptor agonist umbrella. They mimic a hormone your gut naturally produces after you eat. It tells your brain you're full. It slows down your stomach. It makes your pancreas happy. But because these are synthetic versions designed to last way longer than the natural stuff, your nervous system needs time to adjust. If you rush it, you're going to feel it.
The Titration Trap and Why Slow is Smooth
Doctors use a process called "titration." Basically, it’s a fancy word for starting tiny and ramping up. If you look at the clinical trials for semaglutide (the stuff in Wegovy), they didn't just start people at 2.4 mg. No way. They started at 0.25 mg for a full month.
Why? Because your gallbladder and your stomach need to get used to the new speed of things.
When you start a glp-1 dosage for weight loss, the first few weeks are often about "metabolic priming" rather than actual fat loss. Some people lose weight immediately, sure. Others don't see the scale budge until they hit the higher doses. That's totally normal. Dr. Ania Jastreboff at Yale, who has been a lead researcher on many of these trials, often emphasizes that these medications are treating a chronic disease—obesity—and the dosage needs to be managed with a long-term lens. You aren't "failing" if you're on a low dose and only losing a half-pound a week. You're actually letting your body adapt without triggering a massive inflammatory response or severe nausea.
Breaking Down the Standard Schedules
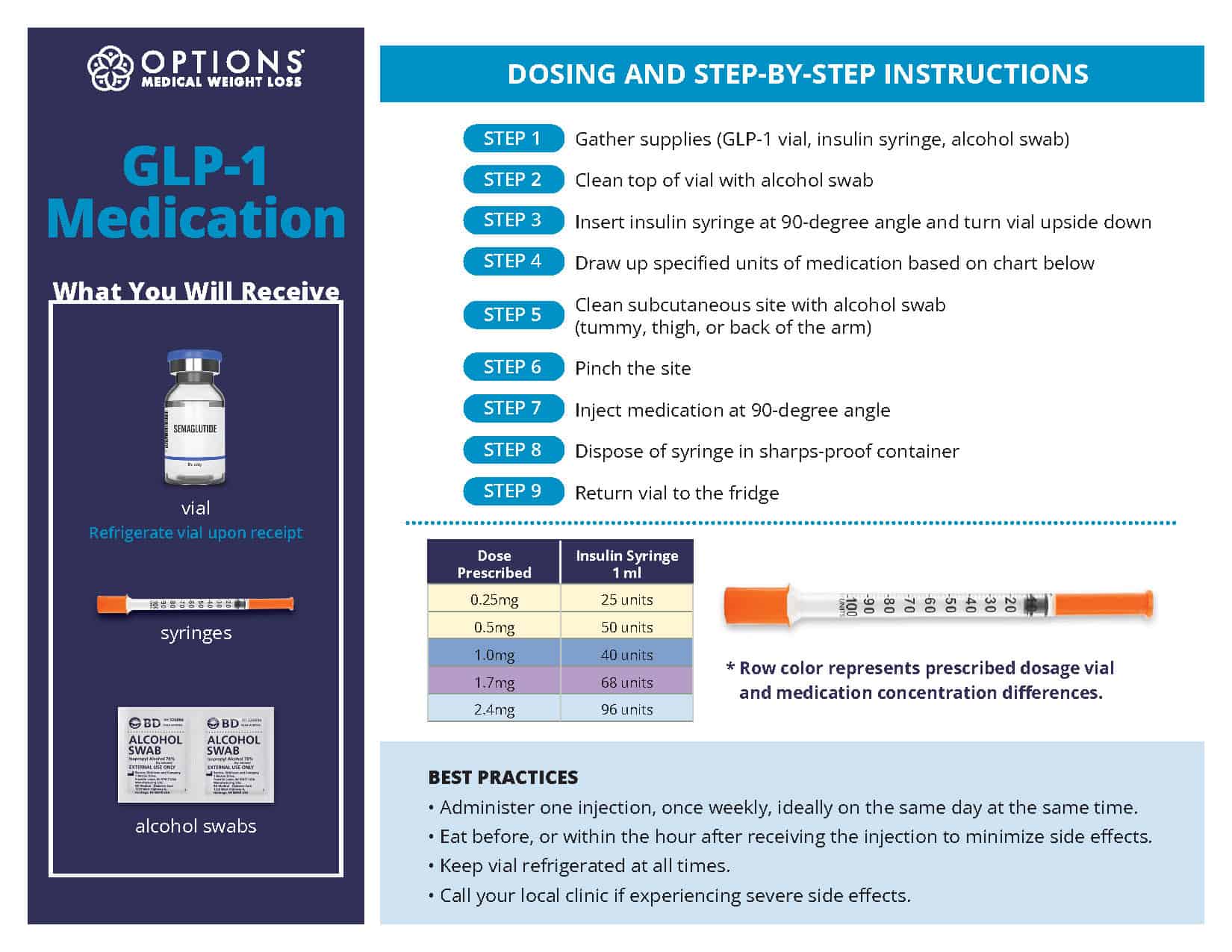
Most GLP-1s follow a 4-week cycle. You take one dose once a week for four weeks, then you bump up. For semaglutide, the ladder usually looks like 0.25 mg, then 0.5 mg, then 1.0 mg, 1.7 mg, and finally the maintenance dose of 2.4 mg.
Tirzepatide (Zepbound) is a bit different because it’s a dual agonist—it hits GLP-1 and GIP receptors. It starts at 2.5 mg and can go all the way up to 15 mg. The GIP component actually helps mitigate some of the nausea, which is why some people find they can handle higher doses of tirzepatide more easily than semaglutide.
But here’s the kicker: just because a dose exists doesn't mean you must reach it.
I’ve talked to plenty of clinicians who say that if a patient is losing 1-2 pounds a week on a mid-level dose and they feel great, there is zero reason to increase the glp-1 dosage for weight loss further. More isn't always better. Sometimes more is just more side effects.
The "Plateau" Panic
Around month three or four, people often hit a wall. The weight loss stops. The "food noise" starts creeping back in. This is usually when the conversation about increasing the dose happens. However, you have to be careful here.
Is it a real plateau, or is your body just catching its breath?
The STEP trials showed that weight loss generally continues for 60+ weeks on a consistent dose. If you hit a two-week stall, that’s not a signal to double your dose. It might just be water weight shifts or your metabolism adjusting to a lower caloric intake. Increasing your glp-1 dosage for weight loss prematurely can lead to "tachyphylaxis," where your body becomes desensitized to the drug faster than it should.
Dealing With the Side Effects of Higher Doses
Nausea. Vomiting. The dreaded "sulfur burps." These aren't just annoyances; they are signs that your current dose might be too high for your gastric emptying rate.
📖 Related: How to Get a Girl Baby: Science, Myths, and What Actually Works
If you're struggling, some doctors suggest staying on a lower dose for an extra month. There’s no law saying you have to move up every four weeks. In fact, many people find a "sweet spot" dose where the hunger is suppressed but they can still actually enjoy a meal with friends. If you can't eat enough protein because your dose is too high, you’ll start losing muscle mass instead of fat. That’s a recipe for a "skinny fat" physique and a ruined metabolism.
- Hydration is non-negotiable: Electrolytes help with the headaches often associated with dose increases.
- Protein first: Aim for 0.8g to 1g of protein per pound of goal body weight.
- Fiber: GLP-1s slow digestion, which can lead to constipation.
Micro-dosing and Compounded Variations
We have to talk about the elephant in the room: the shortages. Because brand-name pens have been so hard to get, many people have turned to compounded versions. This has led to a lot of experimentation with "micro-dosing" or "splitting doses."
While some anecdotal evidence suggests that taking half a dose twice a week can keep blood levels more stable and reduce side effects, the clinical data on this is thin. Most brand-name pens (like Wegovy or Zepbound) are single-use and aren't designed to be split. Attempting to "dose-split" with a single-use pen can lead to contamination or inaccurate dosing.
If you are using a multi-dose vial through a legitimate compounding pharmacy, your glp-1 dosage for weight loss might be measured in "units" on an insulin syringe. This is where people get confused. 0.25 mg is not necessarily 25 units. It depends entirely on the concentration (mg/mL) of the liquid. Always, always double-check the math with your provider. One decimal point error can be the difference between a successful week and an ER visit.
What Happens When You Hit Your Goal?
This is the part nobody talks about. Maintenance.
Do you stay on the max dose forever? Probably not.
Current research, including the SUSTAIN and SURMOUNT trials, suggests that many people need a maintenance dose to keep the weight off. However, that maintenance glp-1 dosage for weight loss is often lower than the peak dose used to lose the weight. Some patients "taper down" to the lowest effective dose that prevents weight regain. Others try spacing their doses out to every 10 or 14 days.
👉 See also: Hepatitis B Vaccine Controversy: What Actually Happened and Why People Still Argue About It
It's a trial-and-error phase. Obesity is a chronic condition, much like hypertension. You wouldn't stop taking blood pressure meds just because your blood pressure is finally normal. The same logic applies here, though the specific dose might change as your body composition stabilizes.
Key Factors That Influence Your Ideal Dose
- Starting BMI: Higher baseline weights sometimes (but not always) require higher doses to see significant movement.
- Insulin Sensitivity: If you have Type 2 diabetes or PCOS, your body might respond differently to the GLP-1 signal.
- Gut Microbiome: Your existing digestive health plays a massive role in how well you tolerate dose escalations.
- Activity Level: High-intensity athletes might find that high doses make them too lethargic to train.
Moving Forward With Your Dosing Plan
If you're just starting out or considering a change, don't rush the process. Your journey with glp-1 dosage for weight loss is unique to your own biology.
Track your symptoms religiously. Keep a log of what you ate, how you felt 24 hours after the injection, and when the hunger suppression starts to fade. This data is gold for your doctor. If the "food noise" returns on day five, your doctor might adjust your schedule rather than just upping the dose.
Prioritize strength training. Since GLP-1 medications can cause significant muscle loss if you aren't careful, the dose you take should allow you enough energy to lift weights. If you're too fatigued to move, the dose is likely too high.
Talk to a specialist. While many primary care doctors can prescribe these, obesity medicine specialists (ABOM certified) often have more experience with nuanced dosing strategies for patients who don't fit the "standard" titration schedule. They can help you navigate the nuances of "non-responders" versus "hyper-responders."
🔗 Read more: Rhinoplasty for Wide Nose Before and After: What Surgeons Don’t Always Tell You
Focus on the long game. The best dose isn't the one that makes the weight fall off the fastest. It’s the one you can sustain for a year or more without ruining your quality of life. Speed is the enemy of skin elasticity and muscle retention. Slow, steady titration wins every single time.