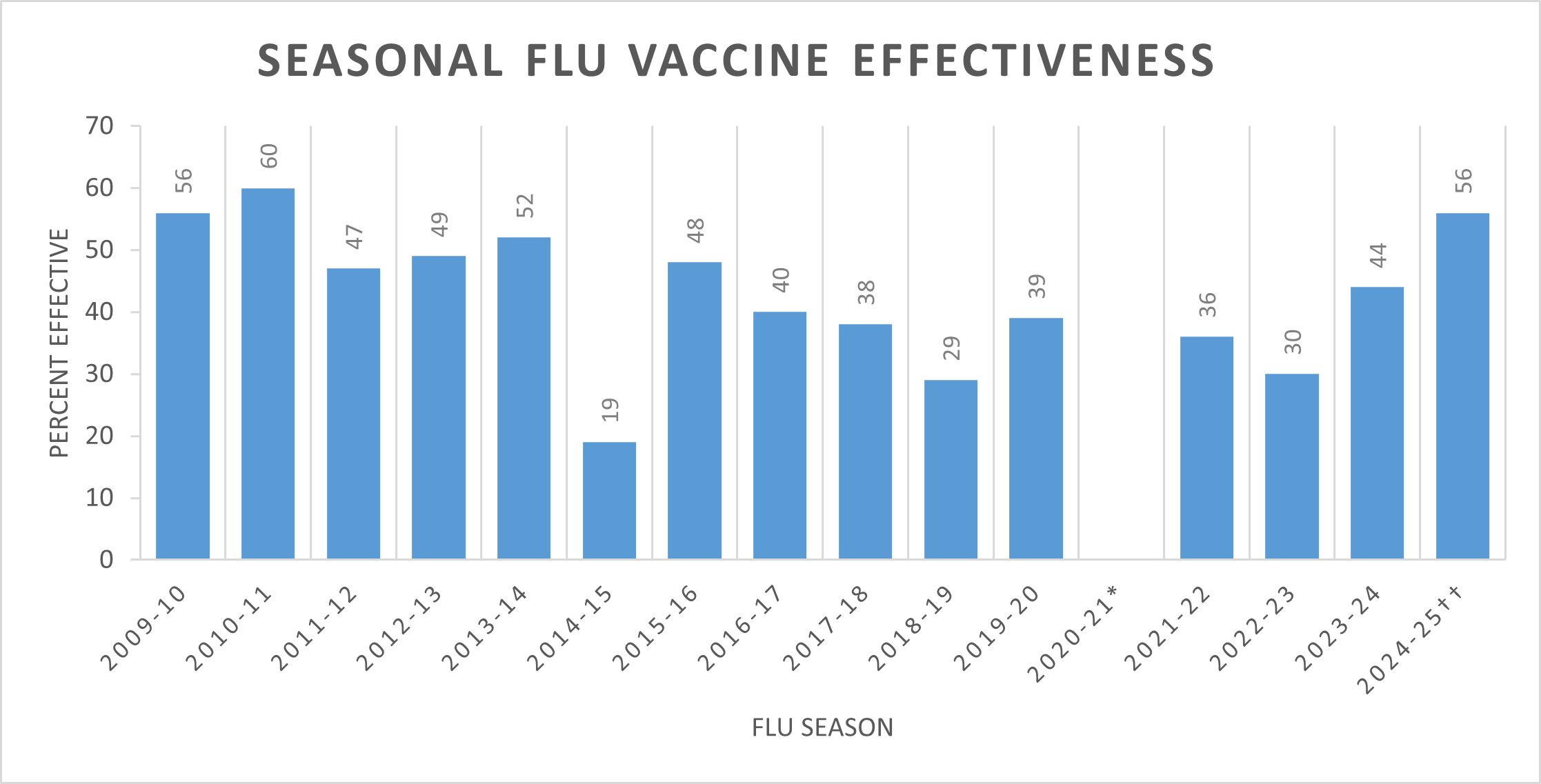
You’ve heard the numbers. Some years they say the shot is 40% effective, others maybe 60%. It sounds like a coin flip, doesn’t it? When people hear "40%," they often think it’s barely worth the trip to the pharmacy. But that’s a massive misunderstanding of how flu vaccine effectiveness actually works in the real world. Honestly, if you're looking at that percentage as a "pass or fail" grade, you're missing the most important part of the data.
Flu season is a moving target. Every year, the World Health Organization (WHO) and the CDC look at what’s circulating in the Southern Hemisphere to predict what will hit us. It's an educated guess. A very, very sophisticated one, but a guess nonetheless. Sometimes the virus mutates—a "mismatch"—and the vaccine isn't a perfect lock-and-key fit.
But here’s the thing. Even a "mismatched" vaccine isn't a zero.
What Flu Vaccine Effectiveness Actually Means (and What It Doesn't)
When researchers talk about "effectiveness," they are usually measuring the "prevention of outpatient medically attended influenza." That’s a fancy way of saying "did this person get sick enough to go to the doctor?" It doesn't account for the person who got a mild sniffle for two days and stayed home watching Netflix.
That person was still protected.
The vaccine’s primary job isn't just to stop you from catching a virus. It’s to keep you out of the hospital. It’s to keep you alive. Think of it like a seatbelt. A seatbelt doesn't prevent a car accident. It prevents you from flying through the windshield when the accident happens.
Data from the CDC consistently shows that even when the flu vaccine effectiveness against infection is lower, its effectiveness against hospitalization and death remains significantly higher. For example, during the 2019-2020 season, flu vaccination prevented an estimated 105,000 hospitalizations. That is a small city's worth of people who stayed out of a hospital bed because of a single shot.
The Nuance of the "Match"
Every February, experts meet to decide which four strains (quadrivalent) should go into the next season's vaccine. They look at H1N1, H3N2, and two B-lineage viruses.
💡 You might also like: That Weird Feeling in Knee No Pain: What Your Body Is Actually Trying to Tell You
H3N2 is the problem child.
It mutates faster than the others. It’s also harder to grow in eggs, which is how most vaccines are still produced. During the "egg-adaptation" process, the virus can actually change slightly, making the final product a bit different from the virus circulating in the wild. This is why some years feel like a "bad match."
If you’re over 65, your immune system doesn't respond as vigorously to a standard shot. That’s just biology. It’s why high-dose vaccines like Fluzone High-Dose or adjuvanted vaccines like Fluad exist. They basically "shout" at the immune system to make sure it's paying attention.
Why Does My Friend Still Get Sick?
We’ve all heard it. "I got the shot and then I got the flu anyway!"
First off, it takes two weeks for the antibodies to kick in. If you get exposed at the pharmacy while waiting for your shot, you're going to get sick. That's not the vaccine failing; that's just bad timing.
Secondly, people call everything "the flu." A bad cold? "The flu." Norovirus (stomach bug)? "The flu." The vaccine only protects against influenza viruses. It does nothing for the 200 other viruses that cause respiratory symptoms.
But let’s say it was the actual flu.
📖 Related: Does Birth Control Pill Expire? What You Need to Know Before Taking an Old Pack
The Severity Gap
A study published in The Lancet Respiratory Medicine looked at vaccinated vs. unvaccinated patients who ended up hospitalized with flu. The vaccinated patients were 59% less likely to be admitted to the ICU. They spent fewer days in the hospital. They were less likely to die.
This is the nuance that gets lost in a 30-second news segment.
If you're vaccinated and you still catch it, your body already has the "wanted poster" for that virus. Your immune system recognizes the intruder and starts fighting immediately. Instead of a week in bed with a 103-degree fever and potential pneumonia, you might have three days of feeling "kinda crummy."
That is a win.
The Communal Math of Viral Spread
We talk a lot about personal protection, but flu vaccine effectiveness is also a numbers game for the community. It’s about "herd immunity," though scientists prefer the term "community immunity" for the flu because it’s so shifty.
When you get vaccinated, you become a dead end for the virus.
If the virus hits you and your immune system kills it before you start shedding enough to infect others, you've protected your grandmother. You've protected the person undergoing chemotherapy at the grocery store. You've protected the infant who is too young to get their own shot.
👉 See also: X Ray on Hand: What Your Doctor is Actually Looking For
Even if the vaccine is only 30% effective at preventing infection, if you vaccinate 100 million people, you have effectively removed 30 million potential "spreaders" from the population. The math adds up fast. It slows the "R naught"—the rate at which the virus replicates through a crowd.
New Tech: Moving Beyond the Egg
For decades, we’ve been stuck in the 1940s using chicken eggs. It’s slow. It’s clunky.
But we’re seeing a shift. Cell-based vaccines (like Flucelvax) and recombinant vaccines (like Flublok) don't use eggs. Flublok, specifically, contains three times the amount of antigen found in a standard dose. Studies suggest it might be more effective in years where the H3N2 strain mutates during egg production.
And then there’s mRNA.
After the success of the COVID-19 vaccines, companies like Moderna and Pfizer are testing mRNA flu shots. The goal? To be able to pivot faster. If a new strain emerges in October, an mRNA platform could theoretically produce a matched vaccine much faster than the months-long egg process. We aren't fully there yet for the general public, but the horizon looks different than it did five years ago.
Misconceptions That Won't Die
- "The shot gave me the flu." No. It’s physically impossible. Injectable flu shots use "killed" viruses or just a single protein. They cannot replicate. You might feel a sore arm or a low-grade fever—that’s just your immune system doing its "practice run."
- "I never get the flu, so I don't need it." You've been lucky. Until you aren't. And you can be asymptomatic and still spread it to someone who isn't as healthy as you.
- "It’s too late in the season." Flu often peaks in February or even March. If it's January and you haven't had it, it's still worth getting.
Practical Steps for Your Next Flu Season
Don't just walk in and ask for "the flu shot." Be a bit more tactical about it.
- Timing is everything. Aim for late September or October. Get it too early (like August), and your immunity might wane before the late-winter peak. Get it too late, and you’re unprotected during the holiday travel surge.
- Know your options. If you’re over 65, insist on the high-dose or adjuvanted version. If you have a severe egg allergy, ask for the cell-based or recombinant versions, though the CDC now says most people with egg allergies can safely get any flu vaccine.
- Check the strains. While you can't pick the strains, you can check the CDC’s weekly "FluView" report to see what’s circulating in your area. If it’s a heavy H3N2 year, being extra cautious with handwashing and masking in crowds—even if you're vaccinated—is a smart move.
- Pair it up. You can get your flu shot and your COVID booster at the same time. One in each arm. It saves a trip and doesn't decrease the effectiveness of either.
- Watch the kids. Children need two doses if it's their first time getting vaccinated. Don't skip that second one; the first one just primes the pump, the second one provides the actual protection.
The reality of flu vaccine effectiveness is that it is a tool, not a shield of invincibility. It is one layer of defense in a complex biological battle that happens every single winter. By reducing the severity of the illness, we keep people out of ICUs and keep the healthcare system from collapsing under the weight of preventable complications. It’s not a perfect system, but it’s the best defense we have against a virus that has been killing humans for centuries.