You’ve probably seen the diagrams. Those neat, white, rope-like bands tucked perfectly behind the kneecap in medical textbooks. They look clean. Simple. Almost like a piece of heavy-duty nylon cord connecting your thigh bone to your shin. But if you’re looking for a picture of the acl because your knee just went "pop" during a pickup game, those drawings aren't going to help you much. Real anatomy is messy. It’s wet, it’s glistening, and honestly, a healthy ACL looks more like a fan of tough, fibrous celery than a single piece of string.
The Anterior Cruciate Ligament (ACL) is the primary stabilizer of your knee. It prevents the tibia (shin bone) from sliding out in front of the femur (thigh bone). When you search for an image of it, you’re usually met with one of three things: a colorful 3D render, a grainy gray MRI slice, or a bright, bloody arthroscopic photo from inside a surgery.
Understanding which one you're looking at is the difference between panic and clarity.
The MRI View: Why It Looks Like a Smudge
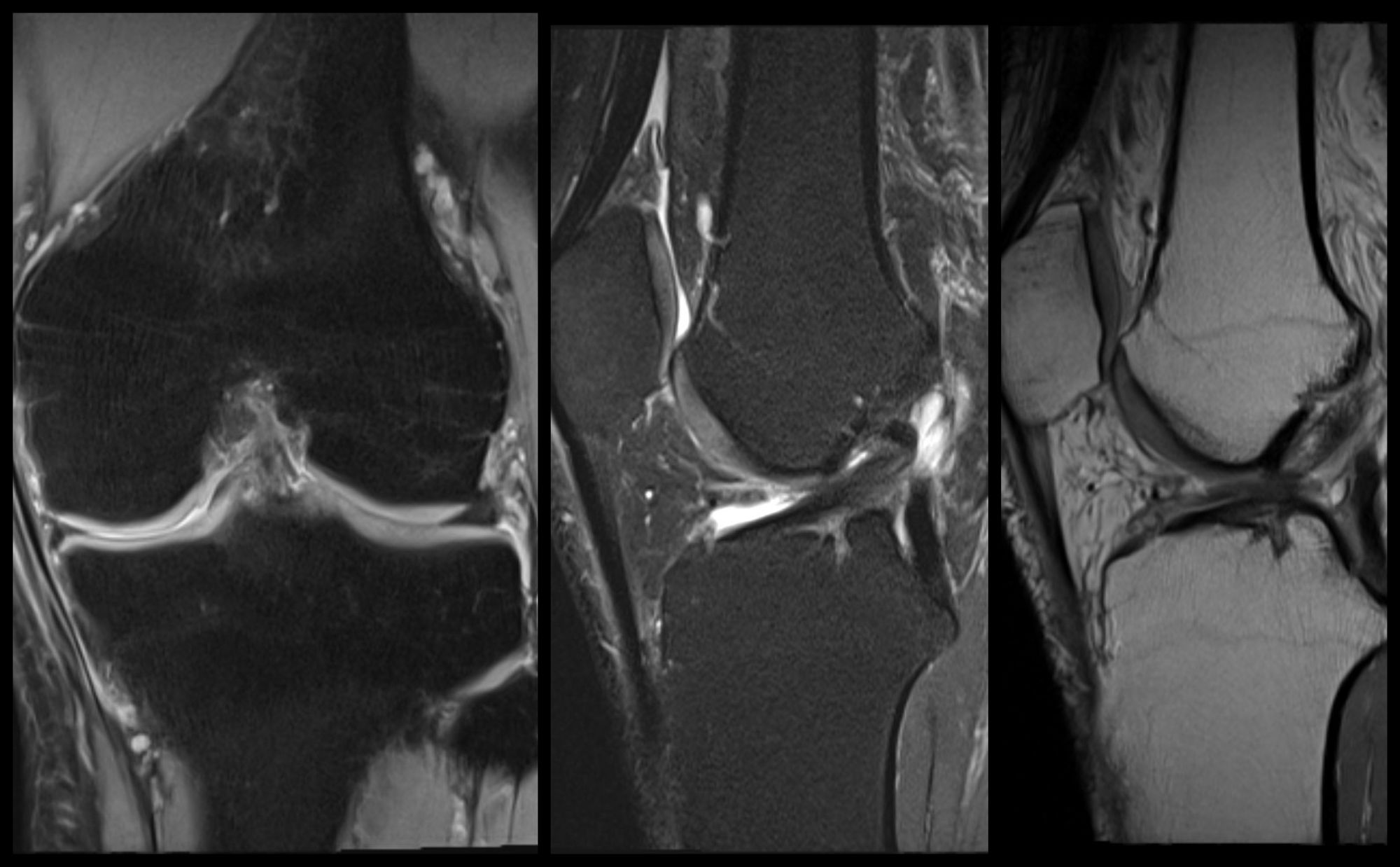
Most people encounter a picture of the acl for the first time on an MRI monitor in a dimly lit doctor’s office. It’s rarely "clear." Radiologists spend years learning how to read these shadows. On a standard T1 or T2-weighted MRI, the ACL shows up as a dark, diagonal band.
It shouldn't be bright white.
If the ligament looks like a "cloud" or a "ghost," that's usually bad news. That blurriness—what doctors call an "increased signal"—often indicates edema or fluid, which is a hallmark of a tear. In a perfect world, a healthy ACL on an MRI looks like a tight, dark ribbon with clear, straight borders. When it’s torn, it looks like a mop head that’s been shredded.
Dr. Robert LaPrade, a world-renowned complex orthopedic knee surgeon, often emphasizes that the ACL isn't just one "thing." It actually has two distinct bundles: the anteromedial and the posterolateral. You can sometimes see these separate strands on high-resolution 3-Tesla MRI images. Most of us just see a dark line. If that line is wavy or sagging, the tension is gone. The "bridge" is down.
Surgery Photos: The Raw Reality
If you’ve ever stumbled upon a picture of the acl taken during an arthroscopy, you’ve seen the real deal. It’s a completely different world. Under the bright lights of a surgical camera, a healthy ACL is a vibrant, pearly white. It has a distinct sheen because it’s covered in a thin layer of synovial tissue.
It’s surprisingly thick.
📖 Related: Does Ginger Ale Help With Upset Stomach? Why Your Soda Habit Might Be Making Things Worse
Think about a piece of licorice. Now imagine that licorice is made of thousands of tiny, individual collagen fibers bundled together. During a "Lachman test"—where a surgeon physically pulls on the bone while looking through the camera—you can see these fibers tighten up like a guitar string. It's beautiful engineering.
When that ligament fails, the visual change is violent. A "mid-substance tear" looks like a bridge that exploded in the middle. The ends become frayed and yellowish. Sometimes, the ligament doesn't snap in the middle but peels off the bone entirely—this is an avulsion. In those pictures, you see a bare patch of bone where the "stump" used to live.
Why a Drawing Isn't a Picture
Medical illustrators do us a huge favor by cleaning things up. In a textbook, the ACL is isolated. In reality? It’s crowded in there. It’s surrounded by the PCL (Posterior Cruciate Ligament), the meniscus (the shock-absorbing pads), and a whole lot of fat pads and lubricating fluid.
You can't just "see" the ACL by looking at your skin.
You’d be surprised how many people think a bruise on the front of the knee is a picture of the acl injury. It’s not. The ACL is deep. It’s the "core" of the joint. By the time blood from a torn ACL reaches the surface to cause a visible bruise, days have usually passed. The real "picture" of the injury is the swelling. If your knee looks like a grapefruit within two hours of an injury, that’s "hemarthrosis." That’s the joint filling with blood because the ACL—which has its own blood supply via the middle genicular artery—has snapped.
The "Empty Notch" Sign
There is a specific picture of the acl that surgeons look for called the "empty notch sign." Inside the femur, there’s a little "U" shaped canyon where the ACL is supposed to sit. When a surgeon moves the camera into that space and sees... nothing? That’s the definitive moment. The ligament has either shriveled up or scarred down to the PCL.
It’s a haunting image for an athlete.
The space is just empty. It’s like looking at a door hinge where the pin has been pulled out. Without that pin, the whole door—or in this case, your leg—just doesn't swing right. It wobbles. It "gives way."
👉 See also: Horizon Treadmill 7.0 AT: What Most People Get Wrong
What Most People Get Wrong About ACL Images
A lot of folks think a partial tear will look like a "half-cut rope" in a picture of the acl. Honestly, it rarely looks that clean. A partial tear often looks like the ligament is still there, but it’s "incompetent." It’s stretched out. It’s like an old rubber band that has lost its snap.
You can’t always see "laxity" in a still photo.
This is why clinical exams matter more than just a single picture. A surgeon needs to feel the "end-point." If they pull your shin forward and it hits a hard stop, the ligament is doing its job. If it feels like pulling a leg through a bowl of oatmeal? No picture is going to change the fact that the ACL is gone.
Seeing the Graft: The "New" ACL
If you’ve had surgery, your new picture of the acl will look different. Most surgeons use a piece of your own patellar tendon or hamstring. This is called an autograft.
- Patellar Tendon Grafts: These look "bony" at the ends because the surgeon actually takes a small plug of bone from your kneecap and shin.
- Hamstring Grafts: These look like several thin strands of spaghetti bundled together with high-strength sutures.
- Allografts: This is tissue from a cadaver. It looks nearly identical to a natural ACL but often lacks that same "pearly" luster initially because it's been processed and frozen.
Over time, something amazing happens. A process called "ligamentization" occurs. Your body crawls onto that new graft and replaces the donor cells with your own. Within a year, a picture of that graft will look remarkably like the original ligament. Nature is a better engineer than we give it credit for.
Why Your "Picture" Might Not Match Your Pain
Here’s a weird fact: some people have a "picture-perfect" ACL on an MRI but their knee feels like it’s falling apart. Others have a "chronic tear" where the ligament looks non-existent on a scan, yet they can run marathons because their muscles are so strong they've taken over the job.
Don't over-index on the image.
The image is just a snapshot. It doesn't show how strong your quadriceps are. It doesn't show your proprioception—your brain's ability to know where your leg is in space. A picture of the acl is a piece of the puzzle, but it isn't the whole story.
✨ Don't miss: How to Treat Uneven Skin Tone Without Wasting a Fortune on TikTok Trends
Practical Next Steps for Your Knee
If you are currently staring at an MRI report or a blurry photo from your doctor, here is exactly what you should do next to move beyond just looking at a picture:
1. Ask for the "Coronal" and "Sagittal" views. The sagittal view is the side profile. It’s the one that looks like a "map" of your knee. If you want to see the ACL's length, that's your go-to. The coronal view looks from the front; it's great for seeing if the ligament is displaced to one side.
2. Look for the "Segond Fracture." Sometimes the best way to see an ACL tear isn't by looking at the ligament itself. Look at the very edge of the tibia. If there’s a tiny chip of bone pulled off, that’s a Segond fracture. It’s almost 100% predictive of an ACL tear, even if the ligament looks "okay" on the scan.
3. Compare it to the "Good" Knee. If you’re looking at your own MRI, ask the tech if you can see a "normal" one for comparison. The difference is usually striking. A healthy ACL has a very specific angle—usually parallel to the "Blumensaat’s line" (the roof of the femoral notch). If the angles don't match, something is wrong.
4. Check the Meniscus. ACL tears rarely travel alone. Look at the "bowties" on the side of the MRI (the menisci). If those bowties are cracked or have white lines through them, you’re dealing with a multi-structure injury.
5. Get a Second Opinion on the "Reading." Radiologists are human. If the report says "equivocal" or "cannot rule out a tear," take those images to an orthopedic surgeon who specializes in sports medicine. They look at these "pictures" all day and often see nuances that a general radiologist might miss.
An ACL injury is a long road, but it starts with understanding the anatomy. Whether you’re looking at a pristine medical illustration or a messy surgical photo, remember that the "picture" is just the starting line for your recovery. Physical therapy and strengthening are the real tools that put the stability back into that frame, regardless of how the ligament looks on a screen.