You’re scrolling. You’re worried. Maybe your lower back has been aching for weeks, or perhaps a sharp, stabbing pain just sent you to the floor during your period. Naturally, you grab your phone and search for a picture of cyst on ovary because you want to know if what’s happening inside you looks like the scary stuff online.
It's a weird feeling, looking at medical imaging. Most people expect to see something obvious, like a bruise or a cut, but ovarian scans are different. They look like grainy, black-and-white weather maps of a storm you can't quite track. Honestly, if you don't know what you're looking at, a perfectly normal follicle can look exactly like a "problem" cyst to the untrained eye.
The reality? Most of the time, those spots are just part of being a person with ovaries. But sometimes, they aren't.
Why that picture of cyst on ovary looks so confusing
When you look at a sonogram, the physics are basically "bounce and return." Sound waves hit something solid, they bounce back white. They hit fluid? They pass right through, appearing as a dark, black void.
A simple cyst is usually just a black circle. It’s a "functional" cyst, meaning it’s likely a follicle that didn't release an egg or a corpus luteum that forgot to shrink. You’ve probably had dozens of these in your life without ever knowing. They come, they go, they cause a little bloat, and then they're gone.
The "Chocolate" Cyst and Complex Scans
Things get visually messy when we talk about complex cysts. If you see a picture of cyst on ovary that looks "cloudy" or has white bits inside it (hyperechoic areas), doctors start paying closer attention.
Endometriomas are a classic example. They get the nickname "chocolate cysts" because they are filled with old, dark blood. On a scan, they don't look like a clear black bubble; they look like ground glass. It’s grainy. It’s dense. These are often markers of endometriosis, a condition where tissue similar to the lining of the uterus grows where it shouldn't. Dr. Linda Giudice, a renowned reproductive endocrinologist, has often highlighted how these specific visual markers help differentiate simple hormonal fluctuations from chronic systemic issues.
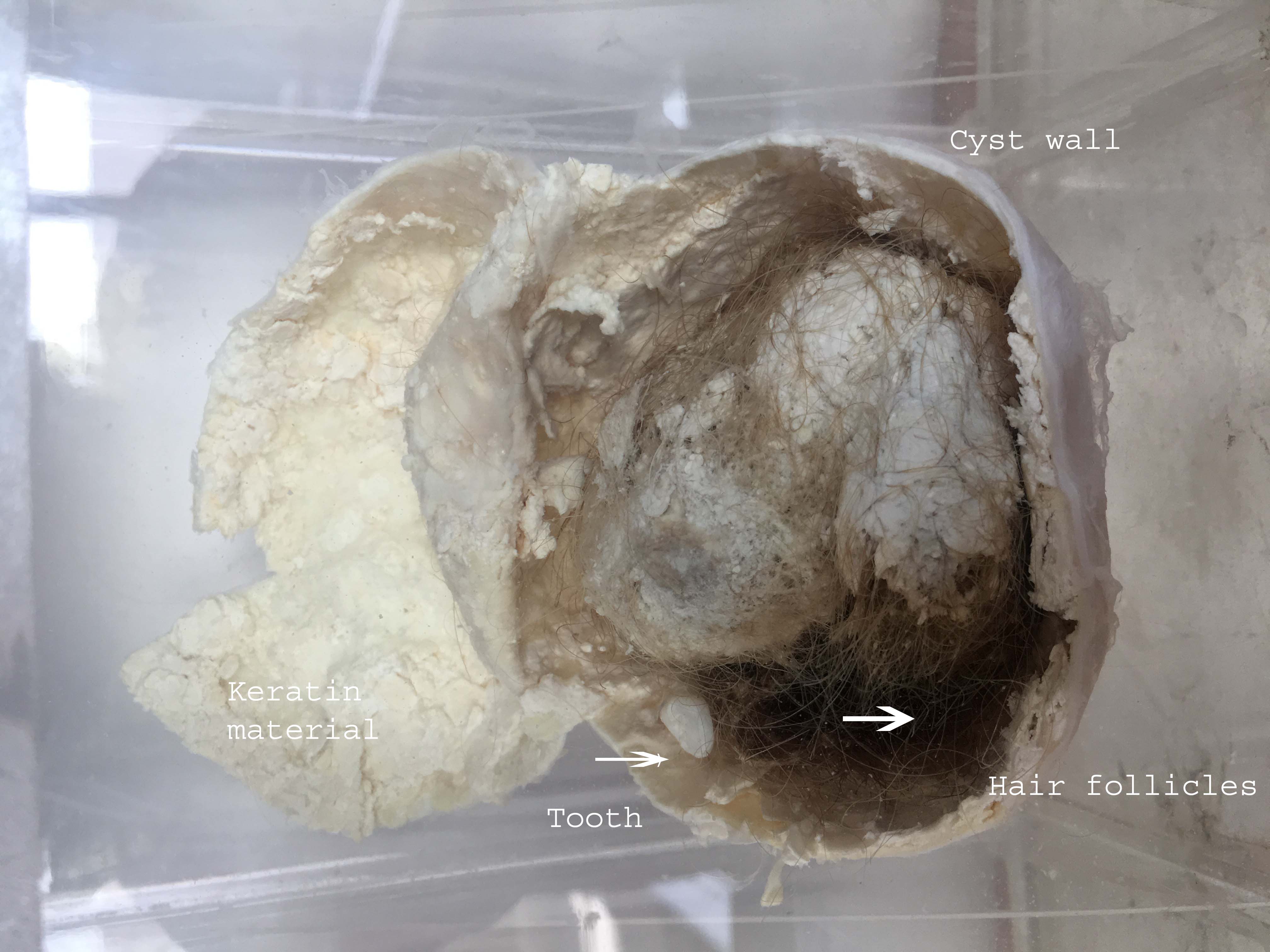
Then you have dermoid cysts. These are the ones that sound like science fiction. They can contain hair, teeth, or skin tissue because they develop from primary germ cells. On a scan, a dermoid looks chaotic. It has solid parts and liquid parts, and it can grow quite large—sometimes larger than a grapefruit.
📖 Related: Does Ginger Ale Help With Upset Stomach? Why Your Soda Habit Might Be Making Things Worse
Spotting the difference: What doctors see vs. what you see
It’s easy to panic when you see a large dark mass on your screen. But size isn't always the indicator of danger. A massive 10cm simple cyst might be less "scary" to a radiologist than a tiny 2cm solid mass with irregular borders.
Vascularity is the big secret here.
During a Doppler ultrasound, the technician isn't just looking at the shape; they are looking at blood flow. If a cyst has blood vessels pumping into its center, that’s a red flag. Benign cysts usually have blood flow around the perimeter, not inside.
- Simple Cysts: Smooth walls, entirely fluid-filled, no internal structures.
- Complex Cysts: Thick walls, internal dividers (septa), or solid "bumps" (mural nodules).
- Hemorrhagic Cysts: Often look like a "spiderweb" inside because of clotted blood strands.
The spiderweb look is actually somewhat reassuring. It usually means a blood vessel in the cyst wall popped, and the body is already starting to break it down. It hurts like hell—often described as a sudden, "take-your-breath-away" pain—but it's usually self-resolving.
The role of CA-125 and the "Innocent" Cyst
We can't talk about the visuals without talking about the bloodwork. Often, if a scan looks suspicious, doctors order a CA-125 test.
Here is the catch: CA-125 is a notoriously "noisy" marker.
It’s a protein that can be elevated if you have ovarian cancer, sure. But it also spikes if you have your period, or if you have a cold, or if you have fibroids. According to researchers at the Mayo Clinic, using CA-125 as a standalone screening tool for premenopausal women often leads to unnecessary surgeries because "normal" things make the numbers jump.
👉 See also: Horizon Treadmill 7.0 AT: What Most People Get Wrong
So, if you see a picture of cyst on ovary that looks a bit murky and your CA-125 is slightly high, it doesn't automatically mean the worst. It means your body is reacting to inflammation. Nuance is everything in gynecology.
When the picture turns into a problem: Torsion and Rupture
Two words every person with a cyst fears.
Torsion happens when the cyst gets so heavy it literally flips the ovary over, cutting off its own blood supply. This is a surgical emergency. The "picture" in this case often shows an enlarged, edematous (swollen) ovary pushed toward the middle of the pelvis.
Rupture is the opposite. The cyst pops. If you had a scan right after a rupture, you might see "free fluid" in the Pouch of Douglas (the space behind the uterus). It’s painful, but unless there’s internal bleeding, the treatment is usually just rest and high-grade ibuprofen.
Beyond the image: What you should actually do
If you are looking at your own scan results or a picture of cyst on ovary from your patient portal, take a breath. Radiologists use a system called O-RADS (Ovarian-Adnexal Reporting and Data System) to categorize how likely a cyst is to be a problem.
- Check the report for the word "Simple": If it's there, you're likely looking at a functional cyst that will vanish in 2-3 cycles.
- Look for "Septations": This means there are walls inside the cyst. Thin walls are usually okay; thick walls need a follow-up.
- Track your cycle: If the pain only happens during ovulation (Mittelschmerz) or right before your period, the cyst is probably following your hormones.
The most important thing? Repeat imaging.
Most doctors will suggest a follow-up scan in 6 to 8 weeks. Why? Because a cancerous growth won't disappear, but a functional cyst will. Time is the best diagnostic tool we have for ovarian health. If the "spot" is gone in two months, you have your answer.
✨ Don't miss: How to Treat Uneven Skin Tone Without Wasting a Fortune on TikTok Trends
Practical steps for your next appointment
Don't just nod when the doctor says "it's probably fine." Ask the specific questions that help you understand the visual data they've collected.
Ask: "Is this a simple or complex cyst?"
Ask: "What was the O-RADS score on the pathology report?"
Ask: "Is there any evidence of internal blood flow or solid components?"
If you're in significant pain and the scan shows a cyst larger than 5cm, discuss the risk of torsion. Sometimes, "watchful waiting" is the right move, but your quality of life matters too. If you can't work or walk because of the pressure, a laparoscopic removal might be on the table regardless of whether the cyst looks "innocent" or not.
Keep your own copies of your scans. Seeing how a picture of cyst on ovary changes over six months is way more valuable than a single snapshot in time. Your body is a moving system, not a still life.
Monitor your symptoms in a journal—not just the pain, but the bloat, the urinary frequency, and the fatigue. Bring that data to your follow-up. When you combine the visual evidence of the scan with the physical evidence of your daily life, you get a much clearer path forward than any Google image search could ever provide.
Next Steps for Your Health:
- Request the formal radiology report: Don't just settle for the doctor's summary. Look for terms like "anechoic" (usually good) or "papillary projections" (needs more investigation).
- Schedule your follow-up for Day 5-10 of your cycle: This is when your ovaries are naturally the "quietest," making it easier to see what is a cyst and what is just a developing follicle.
- Consult a GYN-Oncologist if the O-RADS score is 4 or 5: Even if it's not cancer, these specialists are the absolute experts in complex pelvic surgery and can offer the most nuanced perspective on "messy" scans.