Most people think they know what Parkinson's looks like. You picture an older man, maybe in his 70s, with a hand that won't stop shaking. That’s the classic image. It’s also wildly incomplete. For women, the reality of early Parkinson's symptoms women face is often a lot more subtle, a lot more confusing, and—honestly—frequently dismissed as "just stress" or "perimenopause."
The truth? Parkinson’s is a master of disguise.
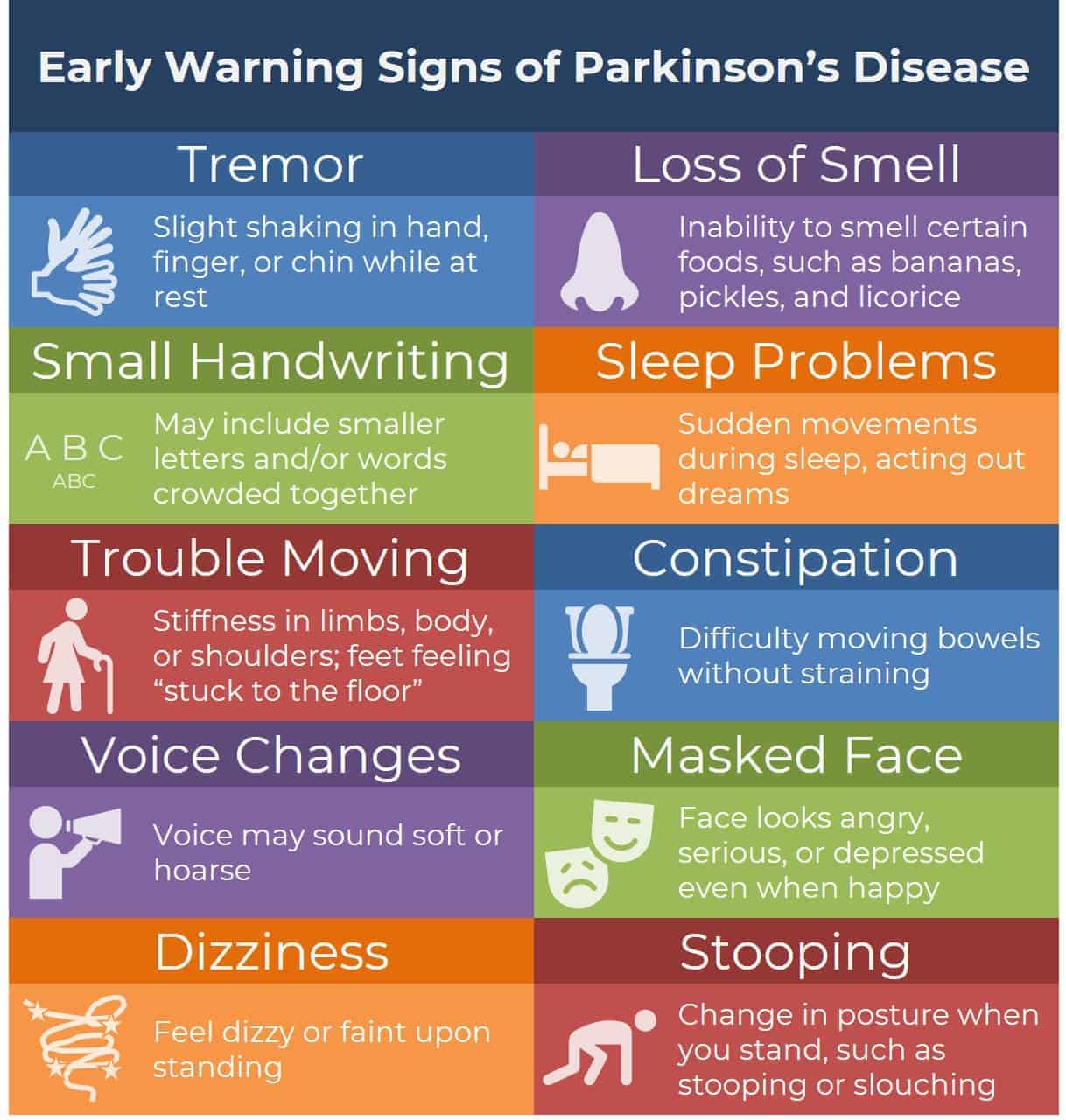
It doesn’t always start with a tremor. In fact, for many women, the very first signs have nothing to do with movement at all. We’re talking about things like losing your sense of smell, feeling a weird sense of anxiety that wasn't there before, or realizing your handwriting has gotten tiny. If you've been feeling "off" and your doctor is telling you it's just your hormones, you aren't crazy. Women often wait longer for a diagnosis than men do, largely because our symptoms don't always fit that "shaky hand" stereotype.
The Hormonal Camouflage: Why Early Parkinson's Symptoms Women Experience Get Missed
The biology of being a woman changes the way this disease shows up. Estrogen is actually thought to be neuroprotective, which is great, but it also creates a bit of a smoke screen. When estrogen levels start to dip during perimenopause or menopause, the early Parkinson's symptoms women notice can suddenly flare up or become much more obvious.
Doctors see a 52-year-old woman complaining of fatigue, sleep issues, and low mood. What’s the first thing they think? Menopause. Every single time.
But there’s a nuance here that gets lost. While menopause causes hot flashes, Parkinson’s-related fatigue is often described as a "heavy" feeling in the limbs, like you're walking through wet concrete. It’s not just being tired; it’s a systemic slowdown. Dr. Rachel Dolhun from the Michael J. Fox Foundation has noted that women often report more non-motor symptoms—things like depression and pain—than their male counterparts. This makes the diagnostic path a total nightmare sometimes.
The "Small" Changes That Actually Matter
Have you noticed your voice getting quieter? It’s called hypophonia. You might think you're just tired, or maybe the room is loud, but your family keeps asking you to repeat yourself. This happens because the muscles involved in speech aren't getting the same "go" signal from the brain.
📖 Related: Orgain Organic Plant Based Protein: What Most People Get Wrong
Then there’s micrographia. That’s just a fancy word for small handwriting. If you look at a thank-you note you wrote five years ago versus one you wrote yesterday, is the script smaller? Are the letters bunched together? This is one of the most reliable early Parkinson's symptoms women and men both experience, yet we rarely think to tell a neurologist about our penmanship.
Movement Isn't Always a Shake
Let's talk about the "non-tremor" movement issues. About 20% of people with Parkinson’s never develop a significant tremor. Instead, they get rigidity.
For a woman, this might feel like a frozen shoulder. You go to physical therapy. You get a cortisone shot. It doesn't get better. Why? Because the problem isn't in the shoulder joint; it's in the basal ganglia of the brain. The brain is sending a constant "contract" signal to the muscle. It’s exhausting.
- Loss of arm swing: Watch yourself walk in a shop window. Does one arm stay glued to your side while the other swings naturally?
- The "Masked Face": Friends might ask if you're upset or bored. Your facial muscles aren't reacting as quickly to your emotions. It's called bradykinesia—slowness of movement.
- Restless Legs: Many women report a creepy-crawly feeling in their legs at night. While Restless Leg Syndrome (RLS) is common on its own, it’s frequently an early warning sign of dopamine changes.
The Gut-Brain Connection and the Nose
This is the part that surprises people the most. The pathology of Parkinson's might actually start in the gut or the olfactory bulb (your nose) years—sometimes a decade—before the first twitch.
Constipation is a massive red flag. We’re not talking about a one-off bad week. We’re talking about a chronic, systemic slowdown of the digestive tract. If you’ve been relying on laxatives for years and you’re starting to feel a bit stiff, it’s time to look at the bigger picture.
And then there's the smell. Anosmia, or the loss of sense of smell, is incredibly common. If you can't smell the coffee brewing or the lilacs in your yard like you used to, pay attention. It’s one of the strongest prodromal (early) indicators we have. Research published in Neurology suggests that people with a reduced sense of smell are significantly more likely to develop Parkinson's within several years.
👉 See also: National Breast Cancer Awareness Month and the Dates That Actually Matter
Anxiety and the Internal Tremor
Women are statistically more likely to be diagnosed with anxiety or depression as an early Parkinson's symptom women present with. But it’s not just "worrying." It’s a chemical shift. Dopamine isn't just for movement; it's a "feel-good" neurotransmitter. When it drops, your mood drops with it.
Many women also describe an "internal tremor." You look perfectly still on the outside. No one can see it. But inside your chest or your limbs, you feel a buzzing or vibrating sensation. It’s incredibly unsettling. Because it's invisible, it often gets written off as a panic attack or generalized anxiety.
Navigating the Path to a Diagnosis
If you suspect something is wrong, you have to be your own advocate. It's frustrating, but it's the reality of the current medical system. Don't just see a general practitioner. You need a Movement Disorder Specialist (MDS). These are neurologists who have extra training specifically in Parkinson's and related conditions.
When you go to your appointment, don't just say "I'm tired." Bring a list.
- "My handwriting has changed."
- "I've lost my sense of smell."
- "My left arm doesn't swing when I walk."
- "I'm experiencing chronic constipation despite a high-fiber diet."
Be specific. Use data. If you have a fitness tracker that shows your sleep is increasingly fragmented or that your "steps" look different, show them.
Real Talk About the "Why"
We still don't fully know why Parkinson's happens. It's a mix of genetics and environment. Maybe it's pesticides. Maybe it's head trauma from years ago. For women, the role of hormones is still being heavily researched. Organizations like PDGENEration are looking into the genetic markers, but for most people, it's "idiopathic"—it just happens.
✨ Don't miss: Mayo Clinic: What Most People Get Wrong About the Best Hospital in the World
The good news? We are living in a golden age of treatment. It’s not a death sentence. It’s a chronic condition that can be managed, often for decades. But the earlier you catch it, the better.
Actionable Next Steps for Women Noticing Changes
If these symptoms feel a bit too familiar, don't panic. Panic doesn't help your dopamine levels anyway. Start with these concrete steps to get clarity.
Track your symptoms for two weeks. Use a simple notebook. Note when you feel "stiff," when your mood dips, and how your sleep is. Look for patterns. Is it worse before your period? Is it constant? This data is gold for a neurologist.
Get a "Smell Test." You can actually ask for formal olfactory testing. If your sense of smell is fine, it doesn't rule out Parkinson's, but if it's gone, it adds a major piece to the puzzle.
Prioritize intense exercise. This is the only thing currently proven to potentially slow the progression of the disease. We’re talking "forced intense" exercise—cycling, boxing (Rock Steady Boxing is a great program), or vigorous walking. If you’re in the early stages, getting your heart rate up is like medicine for your brain.
Check your Vitamin B12 and Vitamin D. Sometimes, deficiencies in these can mimic neurological issues. Rule out the easy stuff first.
Find a Movement Disorder Specialist. Skip the general neurologist if you can. You want someone who sees Parkinson's all day, every day. They are much more likely to recognize the feminine presentation of the disease than a generalist who is looking for a 75-year-old man with a resting tremor.
Listen to your body. You know it better than any clinical textbook. If things feel different, keep pushing until you get an answer that makes sense. Whether it's Parkinson's or something else, you deserve to know why your body is changing. Early intervention is the most powerful tool you have.