If you’ve spent any time searching for dermoid cyst ovary photos, you’ve probably seen some things that look like they belong in a low-budget horror movie rather than a medical textbook. Teeth. Hair. Little bits of bone. Maybe even something that looks suspiciously like brain tissue. It’s deeply weird. Honestly, it’s one of the most bizarre things the human body can do.
These aren't tumors in the way we usually think about them. They aren't just "growths." They are biological time capsules.
Physicians usually call them mature cystic teratomas. That sounds fancy, but "teratoma" actually comes from the Greek word teras, meaning monster. While that’s a bit dramatic for a mostly benign condition, it makes sense once you see the pictures. You’re looking at a collection of tissues that grew in the wrong place because of a developmental glitch. It’s basically a biological "copy-paste" error that happened while you were still an embryo.
What You’re Actually Seeing in Dermoid Cyst Ovary Photos
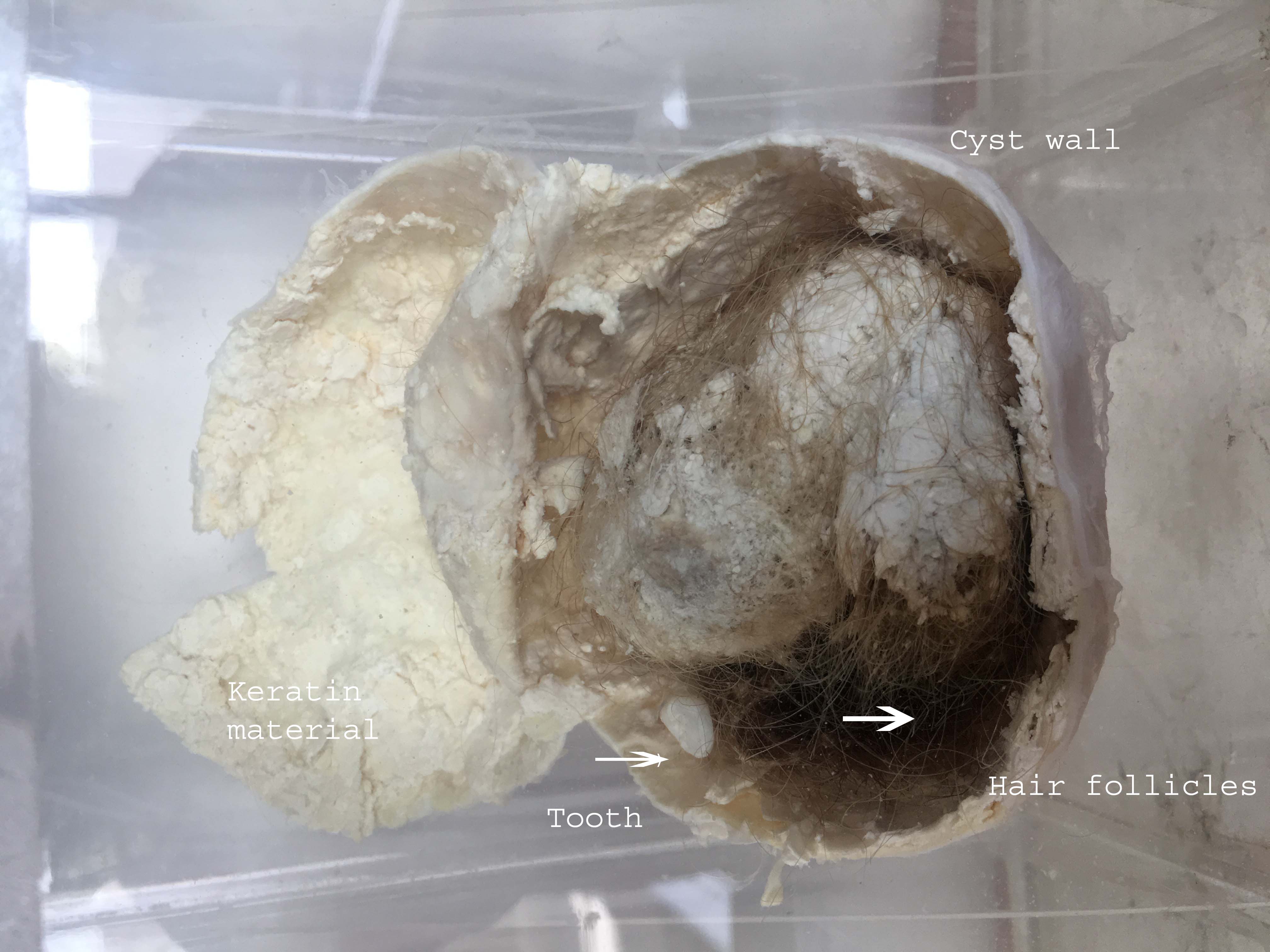
When you look at a photo of a dermoid cyst after it has been surgically removed, the first thing that hits you is the texture. It’s usually a yellowish, fatty mass. This is sebum. It’s the same oil your skin produces, but because it’s trapped inside a closed sac on your ovary, it builds up into a thick, buttery paste.
Most people get hung up on the teeth.
Why are there teeth in an ovary? It’s because these cysts form from germ cells. These are the "master cells" intended to create eggs. Because germ cells are totipotent—meaning they have the potential to turn into any type of tissue in the body—they sometimes get confused. Instead of waiting for fertilization, they just start building. They build skin. They build hair follicles. They build sweat glands.
Sometimes they build a fully formed molar.
📖 Related: Why That Reddit Blackhead on Nose That Won’t Pop Might Not Actually Be a Blackhead
It’s not a twin. That’s a common myth you’ll see in some internet forums, but it’s completely false. There was no pregnancy involved. It’s just your own cells following a scrambled blueprint. Dr. Serene Srouji from Brigham and Women’s Hospital often explains to patients that these tissues are "mature," meaning they are fully developed versions of skin or bone, just misplaced.
The Contrast of Imaging vs. Gross Pathology
There’s a huge difference between the photos taken in an operating room and what you see on an ultrasound.
- The Ultrasound View: Usually, this is the first "photo" a patient sees. It’s grainy. On an ultrasound, a dermoid cyst often shows something called the "Rokitansky protuberance" or a dermoid plug. It looks like a bright white (echogenic) ball sitting inside a darker fluid-filled sac.
- The "Tip of the Iceberg" Sign: This is a classic medical descriptor. Because these cysts contain thick hair and fat, the ultrasound waves can’t pass through them easily. The front of the cyst shows up clearly, but everything behind it is a dark shadow.
- MRI Clarity: If the ultrasound is inconclusive, an MRI provides the high-definition version. MRI photos are incredible at highlighting fat. Since dermoid cysts are loaded with sebaceous material, they "light up" on certain MRI sequences, making the diagnosis almost certain before the surgeon even makes an incision.
Why Doctors Need These Photos for Diagnosis
It’s not just about morbid curiosity. Documenting these cysts through imaging is a matter of surgical precision.
Most of these are benign. About 98% of the time, they aren't cancerous. But they are heavy. Unlike a simple fluid-filled cyst that might resolve on its own, a dermoid cyst is a solid weight. Think of it like a lead sinker on a fishing line. That weight makes the ovary unstable.
This leads to a medical emergency called ovarian torsion.
The ovary twists. The blood supply gets cut off. It’s excruciatingly painful. I’ve talked to women who described the pain as worse than labor. When a surgeon looks at dermoid cyst ovary photos or scans showing a cyst larger than 5 or 6 centimeters, they aren't just looking at a weird growth; they’re looking at a ticking time bomb for torsion.
👉 See also: Egg Supplement Facts: Why Powdered Yolks Are Actually Taking Over
The Complexity of Removal
Surgeons try to use laparoscopy whenever possible. This is "keyhole" surgery. They make tiny cuts and use a camera to see. If you see photos of a cyst being removed this way, you'll notice it’s often placed in a "catch bag" before it’s taken out of the body.
Why the bag?
Because if that cyst ruptures inside the abdomen, all that oily sebum and hair spills out. This can cause a massive inflammatory response called chemical peritonitis. It’s incredibly irritating to the lining of the stomach and can cause long-term scarring or adhesions. So, those photos of the "bagged" cyst are actually showing a critical safety step in the procedure.
Real Life: Beyond the Scary Images
If you’ve just been diagnosed, stop doom-scrolling the grossest photos on Reddit.
Most dermoids are small. Many women go their whole lives without knowing they have one until they get an ultrasound for something else entirely. They grow slowly—usually about 1.8 mm a year.
However, there is a rare complication called a "struma ovarii." This is a dermoid cyst that consists mostly of thyroid tissue. It can actually produce thyroid hormones and cause hyperthyroidism. You could be experiencing heart palpitations and weight loss because of a growth on your ovary. It’s rare, but it’s a perfect example of why these cysts are so fascinating to the medical community. They aren't just "lumps"; they are functional, misplaced organ tissue.
✨ Don't miss: Is Tap Water Okay to Drink? The Messy Truth About Your Kitchen Faucet
Malignant Transformation
We have to talk about the 2%. In older patients, specifically those post-menopause, there is a slight risk that one of the tissues inside the dermoid—usually the skin tissue—can turn into squamous cell carcinoma. This is why doctors don't just "watch and wait" forever with dermoids. If the imaging photos show irregular solid components or sudden rapid growth, the cyst is coming out.
What to Do If You’re Looking at Your Own Scans
If you have your imaging report in hand and you’re seeing terms like "fat-fluid level" or "calcifications," don't panic. Those are actually reassuring terms for a dermoid. They mean the cyst is behaving exactly like a dermoid should.
Next Steps for Patients:
- Consult a Gyn-Oncologist or Specialist: Even if you think it’s benign, seeing a surgeon who specializes in minimally invasive gynecologic surgery (MIGS) is a smart move. They have the best "hands" for removing the cyst while saving the healthy part of your ovary.
- Check Your Markers: Doctors might order blood tests like CA-125. Just a heads up: dermoid cysts can sometimes cause a "false positive" slight elevation in these markers because of inflammation, even if there’s no cancer.
- Track the Pain: If you have a known dermoid and you feel a sudden, sharp, "knock-you-over" pain accompanied by nausea, go to the ER. That’s the sign of torsion.
- Schedule the Surgery: If the cyst is over 5cm, most experts, including those from the American College of Obstetricians and Gynecologists (ACOG), recommend removal. It won't shrink. It won't go away with diet or supplements.
- Preserve Fertility: If you’re in your 20s or 30s, emphasize that you want "cystectomy" (removing just the cyst) rather than "oophorectomy" (removing the whole ovary). In most cases, the remaining ovarian tissue is perfectly healthy and functional.
Dermoid cysts are a weird biological quirk. They represent the incredible, if sometimes confused, power of human cells. Seeing the photos can be jarring, but they are also a roadmap for your surgeon to fix the problem and get your health back on track.
Once the cyst is out, the chance of it coming back in the same ovary is very low—usually less than 3%. You get it removed, you see the crazy photo from the lab, and you move on with a great story to tell at parties (if your friends have a strong stomach).