Walk into any gym in America and you’ll see people obsessing over the scale. They hate that number. But honestly, the scale is a liar. It doesn’t tell you if you’re carrying ten pounds of marble-hard muscle or ten pounds of visceral fat wrapped around your organs. That’s why we need to talk about the average US body fat percentage. It’s a much grittier, more accurate look at how we’re actually doing as a country.
Recent data from the National Health and Nutrition Examination Survey (NHANES) paints a pretty sobering picture. We aren't just getting heavier; our body composition is shifting. It’s not just about "being big." It's about the ratio.
What the Data Actually Says About Us
The numbers are high. Really high. According to the most recent longitudinal studies tracked by the CDC, the average body fat percentage for American men hovers around 28%, while for women, it’s closer to 40%.
Think about that for a second.
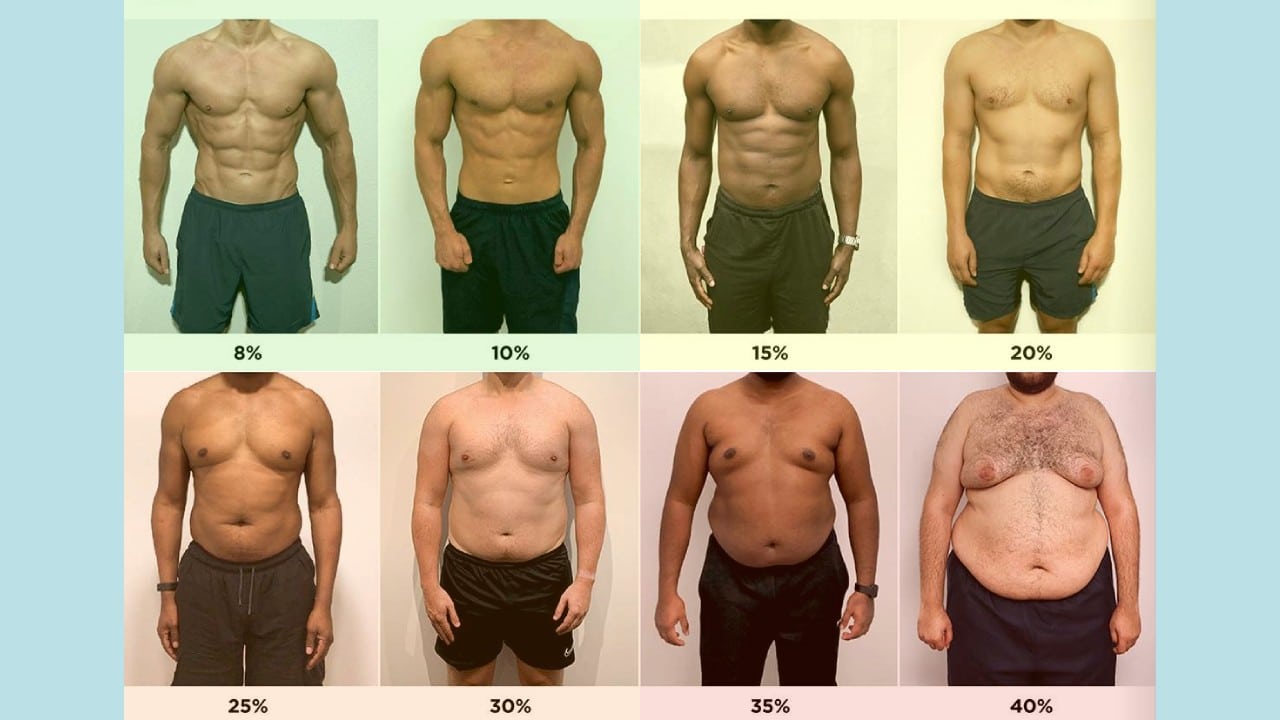
Forty percent. If you’re a woman at that average, nearly half of your physical mass is adipose tissue. For men, 28% is well into the "overweight" or even "obese" category by most clinical standards, like those used by the American Council on Exercise (ACE). ACE generally suggests that for men, a "fitness" range is 14-17%, and for women, it's 21-24%. The gap between where we are and where we "should" be is a massive canyon.
It’s getting wider every year.
Why? Well, it’s not just the fast food. It’s the sedentary jobs. It’s the fact that we sit for eight hours, drive for one, and then sit on the couch for three more. Our bodies are basically storage units for energy we never use.
Age Changes Everything
You can't compare a 22-year-old to a 65-year-old. It’s unfair and scientifically inaccurate. As we age, we hit "sarcopenia." That’s just a fancy medical term for muscle loss. If you don't actively fight to keep your muscle, your body replaces it with fat. Even if the number on the scale stays the same, your body fat percentage creeps up.
A man in his 20s might average 18-20% body fat. By the time he’s 60, that average jumps to 26-30% without him even changing his diet. Women see even sharper spikes, especially around menopause when hormonal shifts—specifically the drop in estrogen—signal the body to start storing more fat in the abdominal area. It’s frustrating. It's biological. But it’s the reality of the average US body fat percentage across different life stages.
The Problem With the "Average"
Average doesn’t mean healthy.
In the United States, "average" is actually a warning sign. Because the majority of the population is now classified as overweight or obese, being average puts you at a significantly higher risk for Type 2 diabetes, hypertension, and non-alcoholic fatty liver disease. Dr. Sean Heffron from NYU Langone Health has often pointed out that it’s the distribution of this fat that really kills us.
Visceral fat is the villain here. This isn't the "pinchable" fat on your arms. This is the stuff packed deep in your belly, crowded around your heart and liver. It’s metabolically active. It pumps out inflammatory cytokines. When we look at the average US body fat percentage, we’re really looking at a nationwide inflammation crisis.
Why BMI Fails Where Body Fat Wins
Everyone uses BMI. Doctors love it because it’s fast. You take the height, you take the weight, you do some quick math, and boom: you’re "Normal," "Overweight," or "Obese."
But it’s kind of a broken system.
Take a professional linebacker. He’s 6'3" and 250 pounds of pure explosive power. His BMI will say he’s morbidly obese. On the flip side, you have "skinny fat" people—individuals with a "normal" BMI who have almost no muscle and a high body fat percentage. These people often have the same metabolic risks as someone who is visibly obese, but they get ignored because their BMI looks fine. Tracking body fat percentage is the only way to catch these hidden risks.
How Do We Even Measure This Stuff?
If you want to know where you stand against the average US body fat percentage, you have a few options. Some are great. Some are basically guessing.
- The DEXA Scan: This is the gold standard. You lie on a table for 10 minutes while a low-level X-ray maps your bone density, muscle, and fat. It’s incredibly accurate. Most universities and high-end clinics offer them for about $100 to $150.
- Bioelectrical Impedance (BIA): These are the scales you stand on at home. They send a tiny electric current through your feet. Water conducts electricity; fat doesn't. They’re "okay" for tracking trends, but they’re notoriously finicky. If you’re dehydrated, the scale will tell you your body fat is way higher than it actually is.
- Skinfold Calipers: This involves a trained pro pinching your fat with a tool. It sounds primitive, but in the hands of someone who knows what they're doing, it’s surprisingly reliable.
- Hydrostatic Weighing: You get dunked in a tank of water. It’s based on Archimedes' principle. It’s accurate but a huge pain in the neck to find a facility that still does it.
Honestly, the DEXA is the way to go if you’re serious. It’s the only way to see if that "weight loss" you’re seeing is actually fat leaving your body or if you’re just losing muscle.
The Lifestyle Factor: Why We Are Where We Are
We live in an "obesogenic" environment. Everything is designed to make us move less and eat more. Our portion sizes have tripled since the 1970s. The average US body fat percentage isn't rising because Americans are "lazy." It’s rising because our environment is rigged.
Think about the "Ultra-Processed Food" (UPF) phenomenon. Studies published in The BMJ have linked high UPF consumption to increased body fat. These foods are designed to bypass our "fullness" signals. You can eat 1,000 calories of potato chips and still feel hungry, but try eating 1,000 calories of steak or broccoli. You can't.
The Muscle Gap
We don't talk enough about the lack of strength training. Most people think "cardio" is the answer to lowering body fat. It helps, sure. But muscle is metabolically expensive. It burns calories just by existing. The average American has less lean muscle mass today than 40 years ago. When you have less muscle, your "basement" for calorie burning is lower. You have to eat less and less just to maintain your weight. It’s a losing battle unless you pick up some weights.
What You Can Actually Do
Don't panic about the averages. Use them as a baseline. If you find out you’re above the average US body fat percentage, the goal isn't to starve yourself. That just causes your body to eat its own muscle, making the percentage problem even worse.
✨ Don't miss: Is Geek Bar FDA Approved? What Most People Get Wrong
Prioritize Protein.
You need roughly 0.7 to 1 gram of protein per pound of your goal body weight. This protects your muscle while you lose fat. If you're 200 pounds and want to be 180, aim for 150-180 grams of protein. It’s hard. It takes effort. But it’s the only way to shift the ratio.
Lift Heavy Things.
Twice a week. That’s the minimum. You don't need to be a bodybuilder. Just do enough to tell your nervous system, "Hey, we need this muscle, don't burn it for fuel." Squats, deadlifts, presses—the basics.
Walk. A lot.
The "10,000 steps" thing is a bit arbitrary, but the logic is sound. Non-Exercise Activity Thermogenesis (NEAT) is the energy you burn doing everything that isn't sleeping, eating, or sports-like exercise. It’s a huge part of your daily burn. Walk while you’re on the phone. Take the stairs. It adds up.
Sleep is Non-Negotiable.
Short-changing your sleep spikes cortisol. High cortisol tells your body to store fat in the belly. You can have a perfect diet and a perfect gym routine, but if you’re only sleeping five hours a night, your body fat percentage will likely stay stuck.
The Realistic Timeline
You didn't reach the average US body fat percentage overnight. You won't drop below it in a week. A healthy rate of fat loss is about 0.5% of total body fat per month. It’s slow. It’s boring. But it’s the only way to make it stick.
Focus on the "Big Three" of body composition:
- Strength training to keep muscle.
- High protein to support that muscle.
- A slight caloric deficit to force the body to use stored fat.
Stop looking at the "average" as the goal. The average American is currently on a path toward chronic illness. Aim for "optimal" instead. Optimal varies by person, but generally, men should aim for 12-20% and women for 20-28%. That’s the "sweet spot" where you feel good, look good, and your bloodwork actually looks healthy.
Track your progress with photos and how your clothes fit. The scale might stay the same for three months while you lose two inches off your waist. That’s a massive win. That’s you beating the average.
Next Steps for Tracking Progress:
- Book a DEXA Scan: Search for a local imaging center or university exercise science department. This gives you a verified starting point.
- Calculate Your Protein Needs: Multiply your goal weight by 0.8. That is your daily gram target.
- Audit Your Movement: Use a wearable or your phone to track your daily steps for one week. If you are under 5,000, aim to increase your daily average by 1,000 steps each week until you hit 8,000-10,000.
- Measure Your Waist: Take a tape measure and check your circumference at the level of your navel. For men, over 40 inches and for women, over 35 inches indicates a high level of visceral fat, regardless of what the scale says.